Warning: The NCBI web site requires JavaScript to function. more...

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.


StatPearls [Internet].
Delivery, face and brow presentation.
Julija Makajeva ; Mohsina Ashraf .
Affiliations
Last Update: January 9, 2023 .
- Continuing Education Activity
Face and brow presentation is a malpresentation during labor when the presenting part is either the face or, in the case of brow presentation, it is the area between the orbital ridge and the anterior fontanelle. This activity reviews the evaluation and management of these two presentations and explains the role of the interprofessional team in managing delivery safely for both the mother and the baby.
- Describe the mechanism of labor in the face and brow presentation.
- Summarize potential maternal and fetal complications during the face and brow presentations.
- Review different management approaches for the face and brow presentation.
- Outline some interprofessional strategies that will improve patient outcomes in delivery cases with face and brow presentation issues.
- Introduction
The term presentation describes the leading part of the fetus or the anatomical structure closest to the maternal pelvic inlet during labor. The presentation can roughly be divided into the following classifications: cephalic, breech, shoulder, and compound. Cephalic presentation is the most common and can be further subclassified as vertex, sinciput, brow, face, and chin. The most common presentation in term labor is the vertex, where the fetal neck is flexed to the chin, minimizing the head circumference.
Face presentation – an abnormal form of cephalic presentation where the presenting part is mentum. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Incidence of face presentation is rare, accounting for approximately 1 in 600 of all presentations. [1] [2] [3]
In brow presentation, the neck is not extended as much as in face presentation, and the leading part is the area between the anterior fontanelle and the orbital ridges. Brow presentation is considered the rarest of all malpresentation with a prevalence of 1 in 500 to 1 in 4000 deliveries. [3]
Both face and brow presentations occur due to extension of the fetal neck instead of flexion; therefore, conditions that would lead to hyperextension or prevent flexion of the fetal neck can all contribute to face or brow presentation. These risk factors may be related to either the mother or the fetus. Maternal risk factors are preterm delivery, contracted maternal pelvis, platypelloid pelvis, multiparity, previous cesarean section, black race. Fetal risk factors include anencephaly, multiple loops of cord around the neck, masses of the neck, macrosomia, polyhydramnios. [2] [4] [5]
These malpresentations are usually diagnosed during the second stage of labor when performing a digital examination. It is possible to palpate orbital ridges, nose, malar eminences, mentum, mouth, gums, and chin in face presentation. Based on the position of the chin, face presentation can be further divided into mentum anterior, posterior, or transverse. In brow presentation, anterior fontanelle and face can be palpated except for the mouth and the chin. Brow presentation can then be further described based on the position of the anterior fontanelle as frontal anterior, posterior, or transverse.
Diagnosing the exact presentation can be challenging, and face presentation may be misdiagnosed as frank breech. To avoid any confusion, a bedside ultrasound scan can be performed. [6] The ultrasound imaging can show a reduced angle between the occiput and the spine or, the chin is separated from the chest. However, ultrasound does not provide much predicting value in the outcome of the labor. [7]
- Anatomy and Physiology
Before discussing the mechanism of labor in the face or brow presentation, it is crucial to highlight some anatomical landmarks and their measurements.
Planes and Diameters of the Pelvis
The three most important planes in the female pelvis are the pelvic inlet, mid pelvis, and pelvic outlet.
Four diameters can describe the pelvic inlet: anteroposterior, transverse, and two obliques. Furthermore, based on the different landmarks on the pelvic inlet, there are three different anteroposterior diameters, named conjugates: true conjugate, obstetrical conjugate, and diagonal conjugate. Only the latter can be measured directly during the obstetric examination. The shortest of these three diameters is obstetrical conjugate, which measures approximately 10.5 cm and is a distance between the sacral promontory and 1 cm below the upper border of the symphysis pubis. This measurement is clinically significant as the fetal head must pass through this diameter during the engagement phase. The transverse diameter measures about 13.5cm and is the widest distance between the innominate line on both sides.
The shortest distance in the mid pelvis is the interspinous diameter and usually is only about 10 cm.
Fetal Skull Diameters
There are six distinguished longitudinal fetal skull diameters:
- Suboccipito-bregmatic: from the center of anterior fontanelle (bregma) to the occipital protuberance, measuring 9.5 cm. This is the presenting diameter in vertex presentation.
- Suboccipito-frontal: from the anterior part of bregma to the occipital protuberance, measuring 10 cm
- Occipito-frontal: from the root of the nose to the most prominent part of the occiput, measuring 11.5cm
- Submento-bregmatic: from the center of the bregma to the angle of the mandible, measuring 9.5 cm. This is the presenting diameter in face presentation where the neck is hyperextended.
- Submento-vertical: from the midpoint between fontanelles and the angle of the mandible, measuring 11.5cm
- Occipito-mental: from the midpoint between fontanelles and the tip of the chin, measuring 13.5 cm. It is the presenting diameter in brow presentation.
Cardinal Movements of Normal Labor
- Neck flexion
- Internal rotation
- Extension (delivers head)
- External rotation (Restitution)
- Expulsion (delivery of anterior and posterior shoulders)
Some of the key movements are not possible in the face or brow presentations.
Based on the information provided above, it is obvious that labor will be arrested in brow presentation unless it spontaneously changes to face or vertex, as the occipito-mental diameter of the fetal head is significantly wider than the smallest diameter of the female pelvis. Face presentation can, however, be delivered vaginally, and further mechanisms of face delivery will be explained in later sections.
- Indications
As mentioned previously, spontaneous vaginal delivery can be successful in face presentation. However, the main indication for vaginal delivery in such circumstances would be a maternal choice. It is crucial to have a thorough conversation with a mother, explaining the risks and benefits of vaginal delivery with face presentation and a cesarean section. Informed consent and creating a rapport with the mother is an essential aspect of safe and successful labor.
- Contraindications
Vaginal delivery of face presentation is contraindicated if the mentum is lying posteriorly or is in a transverse position. In such a scenario, the fetal brow is pressing against the maternal symphysis pubis, and the short fetal neck, which is already maximally extended, cannot span the surface of the maternal sacrum. In this position, the diameter of the head is larger than the maternal pelvis, and it cannot descend through the birth canal. Therefore the cesarean section is recommended as the safest mode of delivery for mentum posterior face presentations.
Attempts to manually convert face presentation to vertex, manual or forceps rotation of the persistent posterior chin to anterior are contraindicated as they can be dangerous.
Persistent brow presentation itself is a contraindication for vaginal delivery unless the fetus is significantly small or the maternal pelvis is large.
Continuous electronic fetal heart rate monitoring is recommended for face and brow presentations, as heart rate abnormalities are common in these scenarios. One study found that only 14% of the cases with face presentation had no abnormal traces on the cardiotocograph. [8] It is advised to use external transducer devices to prevent damage to the eyes. When internal monitoring is inevitable, it is suggested to place monitoring devices on bony parts carefully.
People who are usually involved in the delivery of face/ brow presentation are:
- Experienced midwife, preferably looking after laboring woman 1:1
- Senior obstetrician
- Neonatal team - in case of need for resuscitation
- Anesthetic team - to provide necessary pain control (e.g., epidural)
- Theatre team - in case of failure to progress and an emergency cesarean section will be required.
- Preparation
No specific preparation is required for face or brow presentation. However, it is essential to discuss the labor options with the mother and birthing partner and inform members of the neonatal, anesthetic, and theatre co-ordinating teams.
- Technique or Treatment
Mechanism of Labor in Face Presentation
During contractions, the pressure exerted by the fundus of the uterus on the fetus and pressure of amniotic fluid initiate descent. During this descent, the fetal neck extends instead of flexing. The internal rotation determines the outcome of delivery, if the fetal chin rotates posteriorly, vaginal delivery would not be possible, and cesarean section is permitted. The approach towards mentum-posterior delivery should be individualized, as the cases are rare. Expectant management is acceptable in multiparous women with small fetuses, as a spontaneous mentum-anterior rotation can occur. However, there should be a low threshold for cesarean section in primigravida women or women with large fetuses.
When the fetal chin is rotated towards maternal symphysis pubis as described as mentum-anterior; in these cases further descend through the vaginal canal continues with approximately 73% cases deliver spontaneously. [9] Fetal mentum presses on the maternal symphysis pubis, and the head is delivered by flexion. The occiput is pointing towards the maternal back, and external rotation happens. Shoulders are delivered in the same manner as in vertex delivery.
Mechanism of Labor in Brow Presentation
As this presentation is considered unstable, it is usually converted into a face or an occiput presentation. Due to the cephalic diameter being wider than the maternal pelvis, the fetal head cannot engage; thus, brow delivery cannot take place. Unless the fetus is small or the pelvis is very wide, the prognosis for vaginal delivery is poor. With persistent brow presentation, a cesarean section is required for safe delivery.
- Complications
As the cesarean section is becoming a more accessible mode of delivery in malpresentations, the incidence of maternal and fetal morbidity and mortality during face presentation has dropped significantly. [10]
However, there are still some complications associated with the nature of labor in face presentation. Due to the fetal head position, it is more challenging for the head to engage in the birth canal and descend, resulting in prolonged labor.
Prolonged labor itself can provoke foetal distress and arrhythmias. If the labor arrests or signs of fetal distress appear on CTG, the recommended next step in management is an emergency cesarean section, which in itself carries a myriad of operative and post-operative complications.
Finally, due to the nature of the fetal position and prolonged duration of labor in face presentation, neonates develop significant edema of the skull and face. Swelling of the fetal airway may also be present, resulting in respiratory distress after birth and possible intubation.
- Clinical Significance
During vertex presentation, the fetal head flexes, bringing the chin to the chest, forming the smallest possible fetal head diameter, measuring approximately 9.5cm. With face and brow presentation, the neck hyperextends, resulting in greater cephalic diameters. As a result, the fetal head will engage later, and labor will progress more slowly. Failure to progress in labor is also more common in both presentations compared to vertex presentation.
Furthermore, when the fetal chin is in a posterior position, this prevents further flexion of the fetal neck, as browns are pressing on the symphysis pubis. As a result, descend through the birth canal is impossible. Such presentation is considered undeliverable vaginally and requires an emergency cesarean section.
Manual attempts to change face presentation to vertex, manual or forceps rotation to mentum anterior are considered dangerous and are discouraged.
- Enhancing Healthcare Team Outcomes
A multidisciplinary team of healthcare experts supports the woman and her child during labor and the perinatal period. For a face or brow presentation to be appropriately diagnosed, an experienced midwife and obstetrician must be involved in the vaginal examination and labor monitoring. As fetal anomalies, such as anencephaly or goiter, can contribute to face presentation, sonographers experienced in antenatal scanning should also be involved in the care. It is advised to inform the anesthetic and neonatal teams in advance of the possible need for emergency cesarean section and resuscitation of the neonate. [11] [12]
- Review Questions
- Access free multiple choice questions on this topic.
- Comment on this article.
Disclosure: Julija Makajeva declares no relevant financial relationships with ineligible companies.
Disclosure: Mohsina Ashraf declares no relevant financial relationships with ineligible companies.
This book is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) ( http://creativecommons.org/licenses/by-nc-nd/4.0/ ), which permits others to distribute the work, provided that the article is not altered or used commercially. You are not required to obtain permission to distribute this article, provided that you credit the author and journal.
- Cite this Page Makajeva J, Ashraf M. Delivery, Face and Brow Presentation. [Updated 2023 Jan 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.
In this Page
Bulk download.
- Bulk download StatPearls data from FTP
Related information
- PubMed Links to PubMed
Similar articles in PubMed
- Sonographic diagnosis of fetal head deflexion and the risk of cesarean delivery. [Am J Obstet Gynecol MFM. 2020] Sonographic diagnosis of fetal head deflexion and the risk of cesarean delivery. Bellussi F, Livi A, Cataneo I, Salsi G, Lenzi J, Pilu G. Am J Obstet Gynecol MFM. 2020 Nov; 2(4):100217. Epub 2020 Aug 18.
- Review Sonographic evaluation of the fetal head position and attitude during labor. [Am J Obstet Gynecol. 2022] Review Sonographic evaluation of the fetal head position and attitude during labor. Ghi T, Dall'Asta A. Am J Obstet Gynecol. 2022 Jul 6; . Epub 2022 Jul 6.
- Stages of Labor. [StatPearls. 2024] Stages of Labor. Hutchison J, Mahdy H, Hutchison J. StatPearls. 2024 Jan
- Leopold Maneuvers. [StatPearls. 2024] Leopold Maneuvers. Superville SS, Siccardi MA. StatPearls. 2024 Jan
- Review Labor with abnormal presentation and position. [Obstet Gynecol Clin North Am. ...] Review Labor with abnormal presentation and position. Stitely ML, Gherman RB. Obstet Gynecol Clin North Am. 2005 Jun; 32(2):165-79.
Recent Activity
- Delivery, Face and Brow Presentation - StatPearls Delivery, Face and Brow Presentation - StatPearls
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
What Is Brow Presentation? What Are Its Complications?
What Is Brow Presentation?
What leads to brow presentation, diagnosis of brow presentation, how to avoid c-section if baby is in brow presentation, what complications can arise due to brow presentation.
Unlike the flexed position, in a brow presentation, the baby’s head will not be well flexed into its chest. Therefore, her head and neck will be extended back a little, as if it is looking up. If the baby remains in a brow presentation, it is doubtful that there will be enough space for the baby to descend through the pelvis. This increases the chances of a C-section . Brow presentation is least common of all fetal presentations. In fact, it happens one in every 1400 deliveries. Over half of the babies who are in brow presentation in the early labor will flex their head down during the pushing stage of the labor and the labor may progress as expected. Out of the other 50%, some babies tend to tip their head further back to the face first position while they descends further into the birth canal. Compared to the brow presentation, face first position has a higher chance to undergo a vaginal birth, provided, the chin of the baby is near the pubic bone. But if the baby’s chin is near the tailbone, C-section is the only option to avoid any complications in the delivery. In spite of the fact that brow presentation very rarely happens, it can happen to anybody. If the baby stays in a brow presentation, it is highly unlikely that there will be enough room for it to pass through the pelvis. If the labor is not progressing, or that the baby is becoming distressed, then the doctor will recommend a caesarean delivery.
There are several conditions, which increase the chances of brow presentation. The brow presentation usually takes place because of :
- Polyhydramnios : Excess amniotic fluid can make it difficult for the baby’s head to take a flexed position
- Size and shape of the pelvis: Abnormally shaped and sized pelvis can make it difficult for the baby to pick up a vertex presentation. Android pelvis, which has a triangular or heart-shaped inlet with a narrower front part, is usually behind most of the brow presentations. Similarly, contracted pelvis, a pelvis that is abnormally small, can cause brow presentation
- Fetal abnormality: Fetal abnormalities such as hydrocephalus, anencephaly and neck masses accounts for the majority of brow presentations
- Premature birth/low birth weight baby: If the baby is born prematurely or if the baby is having low birth weight , the chances of brow presentation increases
- Big baby : If the baby is larger than normal size, the baby tends to extend its head instead of curling inward
- Multiple pregnancies: Multiple pregnancies also increase the risk of brow presentation
- Multiple nuchal cords: If the umbilical cord wraps around the baby’s neck, obviously, it cannot tuck its chin into the chest. In such cases, the baby tends to be brow or face presentations
- Laxity of the uterus: If the uterine wall loses its firmness, the baby may not able to hold its chin tucked to the chest firmly and the baby tends to be in brow presentation
- Cephalopelvic disproportion (CPD): If the mother’s pelvis and the baby’s head are not proportionate to each other, brow presentation can happen

When the baby is in brow presentation, the labor will not progress as it should and prolonged labor can result in fetal distress, calling for an immediate C-section. However, if the baby picks up brow presentation and your cervix is fully dilated, there are two procedures through which the doctors try to avoid the need of C-section.
- Manual rotation: Doctor inserts his hand through the cervix and tries to flex the baby’s head
- The baby’s head should be engaged in the pelvis and should be in a front anterior position
- The pelvis should have sufficient room to permit the ventouse cup to be inserted posteriorly and to reach the occiput
- Ability and experience of the obstetrician
- How favorable is the position of the baby’s head inside the pelvis
- Available space inside the pelvis
If both these methods fail, then the doctor will go ahead with the decision to perform a caesarean.
There are several complications associated with a brow presentation if vaginal delivery is attempted without proper measures.
- Increased chances of spinal cord injury are associated with brow presentation
- Fetal distress
- Abnormal shape of the baby’s head after delivery
- Prolonged labor
- Increased chances of using forceps which in turn increases the chances of facial trauma
- Obstructed labor
If it is your first delivery, it is very unlikely that your baby will be in a brow presentation. Also if you had a brow presentation in one delivery, it doesn’t mean that it will definitely happen in your next delivery. Once you are closer to your delivery date, make sure you do not miss any of your doctor appointments.It is advisable to follow your doctor’s instructions from the very beginning of your pregnancy. Make sure you take all precautionary measures to avoid any kind of uneasiness. Have a balanced diet and sufficient rest. Keep yourself positive as you get ready for a healthy delivery . Have a safe and happy pregnancy!

With a rich experience in pregnancy and parenting, our team of experts create insightful, well-curated, and easy-to-read content for our to-be-parents and parents at all stages of parenting.
Related Posts
Occiput posterior position – causes, complications and prevention, two-vessel cord – a high risk pregnancy condition, butterfly exercises to induce labor and easy childbirth.
Save my name, email, and website in this browser for the next time I comment.
Type above and press Enter to search. Press Esc to cancel.
- Getting pregnant
- Preschooler
- Life as a parent
- Baby essentials
- Find your birth club
- Free antenatal classes
- Meet local parents & parents-to-be
- See all in Community
- Ovulation calculator
- Am I pregnant quiz
- How to get pregnant fast
- Best sex positions
- Signs of pregnancy
- How many days after your period can you get pregnant?
- How age affects fertility
- Very early signs of pregnancy
- What fertile cervical mucus looks like
- Think you're pregnant but the test is negative?
- Faint line on pregnancy test
- See all in Getting pregnant
- Pregnancy week by week
- How big is my baby?
- Due date calculator
- Baby movements week by week
- Symptoms you should never ignore
- Hospital bag checklist
- Signs of labour
- Your baby's position in the womb
- Baby gender predictor
- Vaginal spotting
- Fetal development chart
- See all in Pregnancy
- Baby names finder
- Baby name inspiration
- Popular baby names 2022
- Numerology calculator
- Gender-neutral names
- Old-fashioned names
- See all in Baby names
- Your baby week by week
- Baby milestones by month
- Baby rash types
- Baby poop chart
- Ways to soothe a crying baby
- Safe co-sleeping
- Teething signs
- Growth spurts
- See all in Baby
- Your toddler month by month
- Toddler development milestones
- Dealing with tantrums
- Toddler meals
- Food & fussy eating
- When to start potty training
- Moving from a cot to a bed
- Help your child sleep through
- Games & activities
- Vomiting: what's normal?
- See all in Toddler
- Your child month by month
- Food ideas & nutrition
- How kids learn to share
- Coping with aggression
- Bedtime battles
- Anxiety in children
- Dealing with public tantrums
- Great play ideas
- Is your child ready for school?Top tips for starting school
- See all in Preschooler
- Postnatal symptoms to watch out for
- Stitches after birth
- Postpartum blood clots
- Baby showers
- Sex secrets for parents
- See all in Life as a parent
- Best baby products
- Best formula and bottles for a windy baby
- Best car seats if you need three to fit
- Best nappies
- Best Moses baskets
- Best baby registries
- Best baby sleeping bags
- Best baby humidifier
- Best baby monitors
- Best baby bath seat
- Best baby food
- See all in Baby essentials
- Back pain in pregnancy
- Pelvic girdle pain
- Perineal massage
- Signs you're having a boy
- Signs you're having a girl
- Can you take fish oil while pregnant?
- 18 weeks pregnant bump
- Can you eat salami when pregnant?
- Edwards' syndrome
- Missed miscarriage
- Should I harvest my colostrum?
- Rhesus positive vs. Rhesus negative
- What do contractions feel like?
- Hunger in early pregnancy
- First poop after birth
- When do babies sit up?
- When can babies have salt?
- MMR vaccine rash
- Vaping while breastfeeding
- How to transition from formula to milk
- When do babies start grabbing things?
- Sperm allergy: can sperm cause itching?
- How long after taking folic acid can I get pregnant?
What is brow presentation?

- the size or shape of your pelvis
- because your baby is premature
- an abnormality that prevents your baby from tucking in her chin
- having too much amniotic fluid ( polyhydramnios )
Was this article helpful?
My newborn's head is an odd shape. Will it always be like this?

Forceps and ventouse (assisted birth)

Real lives: having triplets

These post-birth photos will take your breath away

Where to go next

Face and Brow Presentation
- Author: Teresa Marino, MD; Chief Editor: Carl V Smith, MD more...
- Sections Face and Brow Presentation
- Mechanism of Labor
- Labor Management
At the onset of labor, assessment of the fetal presentation with respect to the maternal birth canal is critical to the route of delivery. At term, the vast majority of fetuses present in the vertex presentation, where the fetal head is flexed so that the chin is in contact with the fetal thorax. The fetal spine typically lies along the longitudinal axis of the uterus. Nonvertex presentations (including breech, transverse lie, face, brow, and compound presentations) occur in less than 4% of fetuses at term. Malpresentation of the vertex presentation occurs if there is deflexion or extension of the fetal head leading to brow or face presentation, respectively.
In a face presentation, the fetal head and neck are hyperextended, causing the occiput to come in contact with the upper back of the fetus while lying in a longitudinal axis. The presenting portion of the fetus is the fetal face between the orbital ridges and the chin. The fetal chin (mentum) is the point designated for reference during an internal examination through the cervix. The occiput of a vertex is usually hard and has a smooth contour, while the face and brow tend to be more irregular and soft. Like the occiput, the mentum can present in any position relative to the maternal pelvis. For example, if the mentum presents in the left anterior quadrant of the maternal pelvis, it is designated as left mentum anterior (LMA).
In a brow presentation, the fetal head is midway between full flexion (vertex) and hyperextension (face) along a longitudinal axis. The presenting portion of the fetal head is between the orbital ridge and the anterior fontanel. The face and chin are not included. The frontal bones are the point of designation and can present (as with the occiput during a vertex delivery) in any position relative to the maternal pelvis. When the sagittal suture is transverse to the pelvic axis and the anterior fontanel is on the right maternal side, the fetus would be in the right frontotransverse position (RFT).
Face presentation occurs in 1 of every 600-800 live births, averaging about 0.2% of live births. Causative factors associated with a face presentation are similar to those leading to general malpresentation and those that prevent head flexion or favor extension. Possible etiology includes multiple gestations, grand multiparity, fetal malformations, prematurity, and cephalopelvic disproportion. At least one etiological factor may be identified in up to 90% of cases with face presentation.
Fetal anomalies such as hydrocephalus, anencephaly, and neck masses are common risk factors and may account for as many as 60% of cases of face presentation. For example, anencephaly is found in more than 30% of cases of face presentation. Fetal thyromegaly and neck masses also lead to extension of the fetal head.
A contracted pelvis or cephalopelvic disproportion, from either a small pelvis or a large fetus, occurs in 10-40% of cases. Multiparity or a large abdomen can cause decreased uterine tone, leading to natural extension of the fetal head.
Face presentation is diagnosed late in the first or second stage of labor by examination of a dilated cervix. On digital examination, the distinctive facial features of the nose, mouth, and chin, the malar bones, and particularly the orbital ridges can be palpated. This presentation can be confused with a breech presentation because the mouth may be confused with the anus and the malar bones or orbital ridges may be confused with the ischial tuberosities. The facial presentation has a triangular configuration of the mouth to the orbital ridges compared to the breech presentation of the anus and fetal genitalia. During Leopold maneuvers, diagnosis is very unlikely. Diagnosis can be confirmed by ultrasound evaluation, which reveals a hyperextended fetal neck. [ 1 , 2 ]
Brow presentation is the least common of all fetal presentations and the incidence varies from 1 in 500 deliveries to 1 in 1400 deliveries. Brow presentation may be encountered early in labor but is usually a transitional state and converts to a vertex presentation after the fetal neck flexes. Occasionally, further extension may occur resulting in a face presentation.
The causes of a persistent brow presentation are generally similar to those causing a face presentation and include cephalopelvic disproportion or pelvic contracture, increasing parity and prematurity. These are implicated in more than 60% of cases of persistent brow presentation. Premature rupture of membranes may precede brow presentation in as many as 27% of cases.
Diagnosis of a brow presentation can occasionally be made with abdominal palpation by Leopold maneuvers. A prominent occipital prominence is encountered along the fetal back, and the fetal chin is also palpable; however, the diagnosis of a brow presentation is usually confirmed by examination of a dilated cervix. The orbital ridge, eyes, nose, forehead, and anterior fontanelle are palpated. The mouth and chin are not palpable, thus excluding face presentation. Fetal ultrasound evaluation again notes a hyperextended neck.
As with face presentation, diagnosis is often made late in labor with half of cases occurring in the second stage of labor. The most common position is the mentum anterior, which occurs about twice as often as either transverse or posterior positions. A higher cesarean delivery rate occurs with a mentum transverse or posterior [ 3 ] position than with a mentum anterior position.
The mechanism of labor consists of the cardinal movements of engagement, descent, flexion, internal rotation, and the accessory movements of extension and external rotation. Intuitively, the cardinal movements of labor for a face presentation are not completely identical to those of a vertex presentation.
While descending into the pelvis, the natural contractile forces combined with the maternal pelvic architecture allow the fetal head to either flex or extend. In the vertex presentation, the vertex is flexed such that the chin rests on the fetal chest, allowing the suboccipitobregmatic diameter of approximately 9.5 cm to be the widest diameter through the maternal pelvis. This is the smallest of the diameters to negotiate the maternal pelvis. Following engagement in the face presentation, descent is made. The widest diameter of the fetal head negotiating the pelvis is the trachelobregmatic or submentobregmatic diameter, which is 10.2 cm (0.7 cm larger than the suboccipitobregmatic diameter). Because of this increased diameter, engagement does not occur until the face is at +2 station.
Fetuses with face presentation may initially begin labor in the brow position. Using x-ray pelvimetry in a series of 7 patients, Borrell and Ferstrom demonstrated that internal rotation occurs between the ischial spines and the ischial tuberosities, making the chin the presenting part, lower than in the vertex presentation. [ 4 , 5 ] Following internal rotation, the mentum is below the maternal symphysis, and delivery occurs by flexion of the fetal neck. As the face descends onto the perineum, the anterior fetal chin passes under the symphysis and flexion of the head occurs, making delivery possible with maternal expulsive forces.
The above mechanisms of labor in the term infant can occur only if the mentum is anterior and at term, only the mentum anterior face presentation is likely to deliver vaginally. If the mentum is posterior or transverse, the fetal neck is too short to span the length of the maternal sacrum and is already at the point of maximal extension. The head cannot deliver as it cannot extend any further through the symphysis and cesarean delivery is the safest route of delivery.
Fortunately, the mentum is anterior in over 60% of cases of face presentation, transverse in 10-12% of cases, and posterior only 20-25% of the time. Fetuses with the mentum transverse position usually rotate to the mentum anterior position, and 25-33% of fetuses with mentum posterior position rotate to a mentum anterior position. When the mentum is posterior, the neck, head and shoulders must enter the pelvis simultaneously, resulting in a diameter too large for the maternal pelvis to accommodate unless in the very preterm or small infant.
Three labor courses are possible when the fetal head engages in a brow presentation. The brow may convert to a vertex presentation, to a face presentation, or remain as a persistent brow presentation. More than 50% of brow presentations will convert to vertex or face presentation and labor courses are managed accordingly when spontaneous conversion occurs.
In the brow presentation, the occipitomental diameter, which is the largest diameter of the fetal head, is the presenting portion. Descent and internal rotation occur only with an adequate pelvis and if the face can fit under the pubic arch. While the head descends, it becomes wedged into the hollow of the sacrum. Downward pressure from uterine contractions and maternal expulsive forces may cause the mentum to extend anteriorly and low to present at the perineum as a mentum anterior face presentation.
If internal rotation does not occur, the occipitomental diameter, which measures 1.5 cm wider than the suboccipitobregmatic diameter and is thus the largest diameter of the fetal head, presents at the pelvic inlet. The head may engage but can descend only with significant molding. This molding and subsequent caput succedaneum over the forehead can become so extensive that identification of the brow by palpation is impossible late in labor. This may result in a missed diagnosis in a patient who presents later in active labor.
If the mentum is anterior and the forces of labor are directed toward the fetal occiput, flexing the head and pivoting the face under the pubic arch, there is conversion to a vertex occiput posterior position. If the occiput lies against the sacrum and the forces of labor are directed against the fetal mentum, the neck may extend further, leading to a face presentation.
The persistent brow presentation with subsequent delivery only occurs in cases of a large pelvis and/or a small infant. Women with gynecoid pelvis or multiparity may be given the option to labor; however, dysfunctional labor and cephalopelvic disproportion are more likely if this presentation persists.
Labor management of face and brow presentation requires close observation of labor progression because cephalopelvic disproportion, dysfunctional labor, and prolonged labor are much more common. As mentioned above, the trachelobregmatic or submentobregmatic diameters are larger than the suboccipitobregmatic diameter. Duration of labor with a face presentation is generally the same as duration of labor with a vertex presentation, although a prolonged labor may occur. As long as maternal or fetal compromise is not evident, labor with a face presentation may continue. [ 6 ] A persistent mentum posterior presentation is an indication for delivery by cesarean section.
Continuous electronic fetal heart rate monitoring is considered mandatory by many authors because of the increased incidence of abnormal fetal heart rate patterns and/or nonreassuring fetal heart rate patterns. [ 7 ] An internal fetal scalp electrode may be used, but very careful application of the electrode must be ensured. The mentum is the recommended site of application. Facial edema is common and can obscure the fetal facial anatomy and improper placement can lead to facial and ophthalmic injuries. Oxytocin can be used to augment labor using the same precautions as in a vertex presentation and the same criteria of assessment of uterine activity, adequacy of the pelvis, and reassuring fetal heart tracing.
Fetuses with face presentation can be delivered vaginally with overall success rates of 60-70%, while more than 20% of fetuses with face presentation require cesarean delivery. Cesarean delivery is performed for the usual obstetrical indications, including arrest of labor and nonreassuring fetal heart rate pattern.
Attempts to manually convert the face to vertex (Thom maneuver) or to rotate a posterior position to a more favorable anterior mentum position are rarely successful and are associated with high fetal morbidity and mortality and maternal morbidity, including cord prolapse, uterine rupture, and fetal cervical spine injury with neurological impairment. Given the availability and safety of cesarean delivery, internal rotation maneuvers are no longer justified unless cesarean section cannot be readily performed.
Internal podalic version and breech extraction are also no longer recommended in the modern management of the face presentation. [ 8 ]
Operative delivery with forceps must be approached with caution. Since engagement occurs when the face is at +2 position, forceps should only be applied to the face that has caused the perineum to bulge. Increased complications to both mother and fetus can occur [ 9 ] and operative delivery must be approached with caution or reserved when cesarean section is not readily available. Forceps may be used if the mentum is anterior. Although the landmarks are different, the application of any forceps is made as if the fetus were presenting directly in the occiput anterior position. The mouth substitutes for the posterior fontanelle, and the mentum substitutes for the occiput. Traction should be downward to maintain extension until the mentum passes under the symphysis, and then gradually elevated to allow the head to deliver by flexion. During delivery, hyperextension of the fetal head should be avoided.
As previously mentioned, the persistent brow presentation has a poor prognosis for vaginal delivery unless the fetus is small, premature, or the maternal pelvis is large. Expectant management is reasonable if labor is progressing well and the fetal well-being is assessed, as there can be spontaneous conversion to face or vertex presentation. The earlier in labor that brow presentation is diagnosed, the higher the likelihood of conversion. Minimal intervention during labor is recommended and some feel the use of oxytocin in the brow presentation is contraindicated.
The use of operative vaginal delivery or manual conversion of a brow to a more favorable presentation is contraindicated as the risks of perinatal morbidity and mortality are unacceptably high. Prolonged, dysfunctional, and arrest of labor are common, necessitating cesarean section delivery.
The incidence of perinatal morbidity and mortality and maternal morbidity has decreased due to the increased incidence of cesarean section delivery for malpresentation, including face and brow presentation.
Neonates delivered in the face presentation exhibit significant facial and skull edema, which usually resolves within 24-48 hours. Trauma during labor may cause tracheal and laryngeal edema immediately after delivery, which can result in neonatal respiratory distress. In addition, fetal anomalies or tumors, such as fetal goiters that may have contributed to fetal malpresentation, may make intubation difficult. Physicians with expertise in neonatal resuscitation should be present at delivery in the event that intubation is required. When a fetal anomaly has been previously diagnosed by ultrasonographic evaluation, the appropriate pediatric specialists should be consulted and informed at time of labor.
Bellussi F, Ghi T, Youssef A, et al. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol . 2017 Dec. 217 (6):633-41. [QxMD MEDLINE Link] .
[Guideline] Ghi T, Eggebø T, Lees C, et al. ISUOG Practice Guidelines: intrapartum ultrasound. Ultrasound Obstet Gynecol . 2018 Jul. 52 (1):128-39. [QxMD MEDLINE Link] . [Full Text] .
Shaffer BL, Cheng YW, Vargas JE, Laros RK Jr, Caughey AB. Face presentation: predictors and delivery route. Am J Obstet Gynecol . 2006 May. 194(5):e10-2. [QxMD MEDLINE Link] .
Borell U, Fernstrom I. The mechanism of labour. Radiol Clin North Am . 1967 Apr. 5(1):73-85. [QxMD MEDLINE Link] .
Borell U, Fernstrom I. The mechanism of labour in face and brow presentation: a radiographic study. Acta Obstet Gynecol Scand . 1960. 39:626-44.
Gardberg M, Leonova Y, Laakkonen E. Malpresentations--impact on mode of delivery. Acta Obstet Gynecol Scand . 2011 May. 90(5):540-2. [QxMD MEDLINE Link] .
Collaris RJ, Oei SG. External cephalic version: a safe procedure? A systematic review of version-related risks. Acta Obstet Gynecol Scand . 2004 Jun. 83(6):511-8. [QxMD MEDLINE Link] .
Verspyck E, Bisson V, Gromez A, Resch B, Diguet A, Marpeau L. Prophylactic attempt at manual rotation in brow presentation at full dilatation. Acta Obstet Gynecol Scand . 2012 Nov. 91(11):1342-5. [QxMD MEDLINE Link] .
Johnson JH, Figueroa R, Garry D. Immediate maternal and neonatal effects of forceps and vacuum-assisted deliveries. Obstet Gynecol . 2004 Mar. 103(3):513-8. [QxMD MEDLINE Link] .
Benedetti TJ, Lowensohn RI, Truscott AM. Face presentation at term. Obstet Gynecol . 1980 Feb. 55(2):199-202. [QxMD MEDLINE Link] .
BROWNE AD, CARNEY D. OBSTETRICS IN GENERAL PRACTICE. MANAGEMENT OF MALPRESENTATIONS IN OBSTETRICS. Br Med J . 1964 May 16. 1(5393):1295-8. [QxMD MEDLINE Link] .
Campbell JM. Face presentation. Aust N Z J Obstet Gynaecol . 1965 Nov. 5(4):231-4. [QxMD MEDLINE Link] .
Contributor Information and Disclosures
Teresa Marino, MD Assistant Professor, Attending Physician, Division of Maternal-Fetal Medicine, Tufts Medical Center Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference Disclosure: Received salary from Medscape for employment. for: Medscape.
Carl V Smith, MD The Distinguished Chris J and Marie A Olson Chair of Obstetrics and Gynecology, Professor, Department of Obstetrics and Gynecology, Senior Associate Dean for Clinical Affairs, University of Nebraska Medical Center Carl V Smith, MD is a member of the following medical societies: American College of Obstetricians and Gynecologists , American Institute of Ultrasound in Medicine , Association of Professors of Gynecology and Obstetrics , Central Association of Obstetricians and Gynecologists , Society for Maternal-Fetal Medicine , Council of University Chairs of Obstetrics and Gynecology , Nebraska Medical Association Disclosure: Nothing to disclose.
Chitra M Iyer, MD, Perinatologist, Obstetrix Medical Group, Fort Worth, Texas.
Chitra M Iyer, MD is a member of the following medical societies: American College of Obstetricians and Gynecologists , Society of Maternal-Fetal Medicine .
Disclosure: Nothing to disclose.
What would you like to print?
- Print this section
- Print the entire contents of
- Print the entire contents of article
- HIV in Pregnancy
- Pulmonary Disease and Pregnancy
- Kidney Disease and Pregnancy
- Vaccinations/Immunizations During Pregnancy
- Common Pregnancy Complaints and Questions
- Shock and Pregnancy
- Anemia and Thrombocytopenia in Pregnancy
- Is immunotherapy for cancer safe in pregnancy?
- Prenatal Exercise Cuts Common Pregnancy Complications
- Are Nicotine Patches and E-Cigarettes Safe in Pregnancy?

- Drug Interaction Checker
- Pill Identifier
- Calculators

- 2020/viewarticle/immunotherapy-cancer-safe-pregnancy-2024a100083dnews news Is immunotherapy for cancer safe in pregnancy?

- 2002261369-overviewDiseases & Conditions Diseases & Conditions Postterm Pregnancy
- 2002246123-overviewDiseases & Conditions Diseases & Conditions Kidney Disease and Pregnancy
Medical Information

Delivery, Face Presentation, and Brow Presentation: Understanding Fetal Positions and Birth Scenarios
Introduction:.
During childbirth, the position of the baby plays a significant role in the delivery process. While the most common fetal presentation is the head-down position (vertex presentation), variations can occur, such as face presentation and brow presentation. This comprehensive article aims to provide a thorough understanding of delivery, face presentation, and brow presentation, including their definitions, causes, complications, and management approaches.
Delivery Process:
- Normal Vertex Presentation: In a typical delivery, the baby is positioned head-down, with the back of the head (occiput) leading the way through the birth canal.
- Engagement and Descent: Prior to delivery, the baby's head engages in the pelvis and gradually descends, preparing for birth.
- Cardinal Movements: The baby undergoes a series of cardinal movements, including flexion, internal rotation, extension, external rotation, and restitution, which facilitate the passage through the birth canal.
Face Presentation:
- Definition: Face presentation occurs when the baby's face is positioned to lead the way through the birth canal instead of the vertex (head).
- Causes: Face presentation can occur due to factors such as abnormal fetal positioning, multiple pregnancies, uterine abnormalities, or maternal pelvic anatomy.
- Complications: Face presentation is associated with an increased risk of prolonged labor, difficulties in delivery, increased fetal malposition, birth injuries, and the need for instrumental delivery.
- Management: The management of face presentation depends on several factors, including the progression of labor, the size of the baby, and the expertise of the healthcare provider. Options may include closely monitoring the progress of labor, attempting a vaginal delivery with careful maneuvers, or considering a cesarean section if complications arise.
Brow Presentation:
- Definition: Brow presentation occurs when the baby's head is partially extended, causing the brow (forehead) to lead the way through the birth canal.
- Causes: Brow presentation may result from abnormal fetal positioning, poor engagement of the fetal head, or other factors that prevent full flexion or extension.
- Complications: Brow presentation is associated with a higher risk of prolonged labor, difficulty in descent, increased chances of fetal head entrapment, birth injuries, and the potential need for instrumental delivery or cesarean section.
- Management: The management of brow presentation depends on various factors, such as cervical dilation, progress of labor, fetal size, and the presence of complications. Close monitoring, expert assessment, and a multidisciplinary approach may be necessary to determine the safest delivery method, which can include vaginal delivery with careful maneuvers, instrumental assistance, or cesarean section if warranted.
Delivery Techniques and Intervention:
- Obstetric Maneuvers: In certain situations, skilled healthcare providers may use obstetric maneuvers, such as manual rotation or the use of forceps or vacuum extraction, to facilitate delivery, reposition the baby, or prevent complications.
- Cesarean Section: In cases where vaginal delivery is not possible or poses risks to the mother or baby, a cesarean section may be performed to ensure a safe delivery.
Conclusion:
Delivery, face presentation, and brow presentation are important aspects of childbirth that require careful management and consideration. Understanding the definitions, causes, complications, and appropriate management approaches associated with these fetal positions can help healthcare providers ensure safe and successful deliveries. Individualized care, close monitoring, and multidisciplinary collaboration are crucial in optimizing maternal and fetal outcomes during these unique delivery scenarios.
Hashtags: #Delivery #FacePresentation #BrowPresentation #Childbirth #ObstetricDelivery
On the Article

Krish Tangella MD, MBA

Alexander Enabnit

Alexandra Warren
Please log in to post a comment.
Related Articles
Test your knowledge, asked by users, related centers, related specialties, related physicians, related procedures, related resources, join dovehubs.
and connect with fellow professionals
Related Directories
At DoveMed, our utmost priority is your well-being. We are an online medical resource dedicated to providing you with accurate and up-to-date information on a wide range of medical topics. But we're more than just an information hub - we genuinely care about your health journey. That's why we offer a variety of products tailored for both healthcare consumers and professionals, because we believe in empowering everyone involved in the care process. Our mission is to create a user-friendly healthcare technology portal that helps you make better decisions about your overall health and well-being. We understand that navigating the complexities of healthcare can be overwhelming, so we strive to be a reliable and compassionate companion on your path to wellness. As an impartial and trusted online resource, we connect healthcare seekers, physicians, and hospitals in a marketplace that promotes a higher quality, easy-to-use healthcare experience. You can trust that our content is unbiased and impartial, as it is trusted by physicians, researchers, and university professors around the globe. Importantly, we are not influenced or owned by any pharmaceutical, medical, or media companies. At DoveMed, we are a group of passionate individuals who deeply care about improving health and wellness for people everywhere. Your well-being is at the heart of everything we do.
For Patients
For professionals, for partners.
Fetal Presentation, Position, and Lie (Including Breech Presentation)
- Key Points |
Abnormal fetal lie or presentation may occur due to fetal size, fetal anomalies, uterine structural abnormalities, multiple gestation, or other factors. Diagnosis is by examination or ultrasonography. Management is with physical maneuvers to reposition the fetus, operative vaginal delivery , or cesarean delivery .
Terms that describe the fetus in relation to the uterus, cervix, and maternal pelvis are
Fetal presentation: Fetal part that overlies the maternal pelvic inlet; vertex (cephalic), face, brow, breech, shoulder, funic (umbilical cord), or compound (more than one part, eg, shoulder and hand)
Fetal position: Relation of the presenting part to an anatomic axis; for vertex presentation, occiput anterior, occiput posterior, occiput transverse
Fetal lie: Relation of the fetus to the long axis of the uterus; longitudinal, oblique, or transverse
Normal fetal lie is longitudinal, normal presentation is vertex, and occiput anterior is the most common position.
Abnormal fetal lie, presentation, or position may occur with
Fetopelvic disproportion (fetus too large for the pelvic inlet)
Fetal congenital anomalies
Uterine structural abnormalities (eg, fibroids, synechiae)
Multiple gestation
Several common types of abnormal lie or presentation are discussed here.

Transverse lie
Fetal position is transverse, with the fetal long axis oblique or perpendicular rather than parallel to the maternal long axis. Transverse lie is often accompanied by shoulder presentation, which requires cesarean delivery.
Breech presentation
There are several types of breech presentation.
Frank breech: The fetal hips are flexed, and the knees extended (pike position).
Complete breech: The fetus seems to be sitting with hips and knees flexed.
Single or double footling presentation: One or both legs are completely extended and present before the buttocks.
Types of breech presentations
|
Breech presentation makes delivery difficult ,primarily because the presenting part is a poor dilating wedge. Having a poor dilating wedge can lead to incomplete cervical dilation, because the presenting part is narrower than the head that follows. The head, which is the part with the largest diameter, can then be trapped during delivery.
Additionally, the trapped fetal head can compress the umbilical cord if the fetal umbilicus is visible at the introitus, particularly in primiparas whose pelvic tissues have not been dilated by previous deliveries. Umbilical cord compression may cause fetal hypoxemia.

Predisposing factors for breech presentation include
Preterm labor
Uterine abnormalities
Fetal anomalies
If delivery is vaginal, breech presentation may increase risk of
Umbilical cord prolapse
Birth trauma
Perinatal death

Face or brow presentation
In face presentation, the head is hyperextended, and position is designated by the position of the chin (mentum). When the chin is posterior, the head is less likely to rotate and less likely to deliver vaginally, necessitating cesarean delivery.
Brow presentation usually converts spontaneously to vertex or face presentation.
Occiput posterior position
The most common abnormal position is occiput posterior.
The fetal neck is usually somewhat deflexed; thus, a larger diameter of the head must pass through the pelvis.
Progress may arrest in the second phase of labor. Operative vaginal delivery or cesarean delivery is often required.
Position and Presentation of the Fetus
Toward the end of pregnancy, the fetus moves into position for delivery. Normally, the presentation is vertex (head first), and the position is occiput anterior (facing toward the pregnant patient's spine) with the face and body angled to one side and the neck flexed. Abnormal presentations include face, brow, breech, and shoulder. Occiput posterior position (facing toward the pregnant patient's pubic bone) is less common than occiput anterior position. |
If a fetus is in the occiput posterior position, operative vaginal delivery or cesarean delivery is often required.
In breech presentation, the presenting part is a poor dilating wedge, which can cause the head to be trapped during delivery, often compressing the umbilical cord.
For breech presentation, usually do cesarean delivery at 39 weeks or during labor, but external cephalic version is sometimes successful before labor, usually at 37 or 38 weeks.

Copyright © 2024 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
- Cookie Preferences

7.10 Brow presentation
Brow presentation constitutes an absolute foeto-pelvic disproportion, and vaginal delivery is impossible (except with preterm birth or extremely low birth weight).
This is an obstetric emergency, because labour is obstructed and there is a risk of uterine rupture and foetal distress.
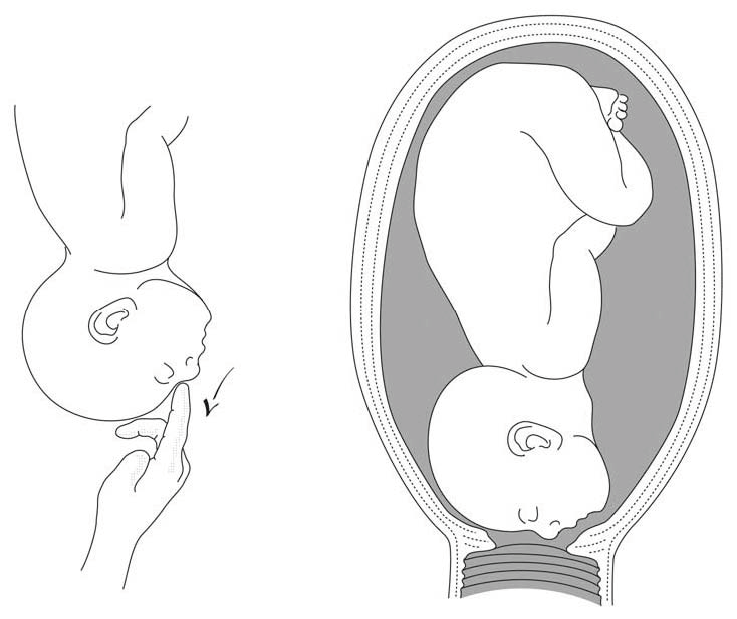
7.10.1 Diagnosis
- Head is high; as with a face presentation, there is a cleft between the head and back, but it is less marked.
- the chin (it is not a face presentation),
- the posterior fontanelle (it is not a vertex presentation).
Figures 7.9 - Brow presentation

Any mobile presenting part can subsequently flex. The diagnosis of brow presentation is, therefore, not made until after the membranes have ruptured and the head has begun to engage in a fixed presentation. Some brow presentations will spontaneously convert to a vertex or, more rarely, a face presentation.
During delivery, the presenting part is slow to descend: the brow is becoming impacted.
7.10.2 Management
Foetus alive.
- Perform a caesarean section. When performing the caesarean section, an assistant must be ready to free the head by pushing it upward with a hand in the vagina.
- Convert the brow presentation to a face presentation: between contractions, insert the fingers through the cervix and move the head, encouraging extension (Figures 7.10).
- Attempt internal podalic version ( Section 7.9 ).
Both these manoeuvres pose a significant risk of uterine rupture. Vacuum extraction, forceps and symphysiotomy are contra-indicated.
Foetus dead
Perform an embryotomy if the cervix is sufficiently dilated (Chapter 9, Section 9.7 ) otherwise, a caesarean section.

- Physician Physician Board Reviews Physician Associate Board Reviews CME Lifetime CME Free CME MATE and DEA Compliance
- Student USMLE Step 1 USMLE Step 2 USMLE Step 3 COMLEX Level 1 COMLEX Level 2 COMLEX Level 3 96 Medical School Exams Student Resource Center NCLEX - RN NCLEX - LPN/LVN/PN 24 Nursing Exams
- Nurse Practitioner APRN/NP Board Reviews CNS Certification Reviews CE - Nurse Practitioner FREE CE
- Nurse RN Certification Reviews CE - Nurse FREE CE
- Pharmacist Pharmacy Board Exam Prep CE - Pharmacist
- Allied Allied Health Exam Prep Dentist Exams CE - Social Worker CE - Dentist
- Point of Care
- Free CME/CE
Delivery, Face and Brow Presentation
Introduction.
The term presentation describes the leading part of the fetus or the anatomical structure closest to the maternal pelvic inlet during labor. The presentation can roughly be divided into the following classifications: cephalic, breech, shoulder, and compound. Cephalic presentation is the most common and can be further subclassified as vertex, sinciput, brow, face, and chin. The most common presentation in term labor is the vertex, where the fetal neck is flexed to the chin, minimizing the head circumference.
Face presentation – an abnormal form of cephalic presentation where the presenting part is mentum. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Incidence of face presentation is rare, accounting for approximately 1 in 600 of all presentations. [1] [2] [3]
In brow presentation, the neck is not extended as much as in face presentation, and the leading part is the area between the anterior fontanelle and the orbital ridges. Brow presentation is considered the rarest of all malpresentation with a prevalence of 1 in 500 to 1 in 4000 deliveries. [3]
Both face and brow presentations occur due to extension of the fetal neck instead of flexion; therefore, conditions that would lead to hyperextension or prevent flexion of the fetal neck can all contribute to face or brow presentation. These risk factors may be related to either the mother or the fetus. Maternal risk factors are preterm delivery, contracted maternal pelvis, platypelloid pelvis, multiparity, previous cesarean section, black race. Fetal risk factors include anencephaly, multiple loops of cord around the neck, masses of the neck, macrosomia, polyhydramnios. [2] [4] [5]
These malpresentations are usually diagnosed during the second stage of labor when performing a digital examination. It is possible to palpate orbital ridges, nose, malar eminences, mentum, mouth, gums, and chin in face presentation. Based on the position of the chin, face presentation can be further divided into mentum anterior, posterior, or transverse. In brow presentation, anterior fontanelle and face can be palpated except for the mouth and the chin. Brow presentation can then be further described based on the position of the anterior fontanelle as frontal anterior, posterior, or transverse.
Diagnosing the exact presentation can be challenging, and face presentation may be misdiagnosed as frank breech. To avoid any confusion, a bedside ultrasound scan can be performed. [6] The ultrasound imaging can show a reduced angle between the occiput and the spine or, the chin is separated from the chest. However, ultrasound does not provide much predicting value in the outcome of the labor. [7]
Anatomy and Physiology
Register for free and read the full article, learn more about a subscription to statpearls point-of-care.
Before discussing the mechanism of labor in the face or brow presentation, it is crucial to highlight some anatomical landmarks and their measurements.
Planes and Diameters of the Pelvis
The three most important planes in the female pelvis are the pelvic inlet, mid pelvis, and pelvic outlet.
Four diameters can describe the pelvic inlet: anteroposterior, transverse, and two obliques. Furthermore, based on the different landmarks on the pelvic inlet, there are three different anteroposterior diameters, named conjugates: true conjugate, obstetrical conjugate, and diagonal conjugate. Only the latter can be measured directly during the obstetric examination. The shortest of these three diameters is obstetrical conjugate, which measures approximately 10.5 cm and is a distance between the sacral promontory and 1 cm below the upper border of the symphysis pubis. This measurement is clinically significant as the fetal head must pass through this diameter during the engagement phase. The transverse diameter measures about 13.5cm and is the widest distance between the innominate line on both sides.
The shortest distance in the mid pelvis is the interspinous diameter and usually is only about 10 cm.
Fetal Skull Diameters
There are six distinguished longitudinal fetal skull diameters:
- Suboccipito-bregmatic: from the center of anterior fontanelle (bregma) to the occipital protuberance, measuring 9.5 cm. This is the presenting diameter in vertex presentation.
- Suboccipito-frontal: from the anterior part of bregma to the occipital protuberance, measuring 10 cm
- Occipito-frontal: from the root of the nose to the most prominent part of the occiput, measuring 11.5cm
- Submento-bregmatic: from the center of the bregma to the angle of the mandible, measuring 9.5 cm. This is the presenting diameter in face presentation where the neck is hyperextended.
- Submento-vertical: from the midpoint between fontanelles and the angle of the mandible, measuring 11.5cm
- Occipito-mental: from the midpoint between fontanelles and the tip of the chin, measuring 13.5 cm. It is the presenting diameter in brow presentation.
Cardinal Movements of Normal Labor
- Neck flexion
- Internal rotation
- Extension (delivers head)
- External rotation (Restitution)
- Expulsion (delivery of anterior and posterior shoulders)
Some of the key movements are not possible in the face or brow presentations.
Based on the information provided above, it is obvious that labor will be arrested in brow presentation unless it spontaneously changes to face or vertex, as the occipito-mental diameter of the fetal head is significantly wider than the smallest diameter of the female pelvis. Face presentation can, however, be delivered vaginally, and further mechanisms of face delivery will be explained in later sections.
Indications
As mentioned previously, spontaneous vaginal delivery can be successful in face presentation. However, the main indication for vaginal delivery in such circumstances would be a maternal choice. It is crucial to have a thorough conversation with a mother, explaining the risks and benefits of vaginal delivery with face presentation and a cesarean section. Informed consent and creating a rapport with the mother is an essential aspect of safe and successful labor.
Contraindications
Vaginal delivery of face presentation is contraindicated if the mentum is lying posteriorly or is in a transverse position. In such a scenario, the fetal brow is pressing against the maternal symphysis pubis, and the short fetal neck, which is already maximally extended, cannot span the surface of the maternal sacrum. In this position, the diameter of the head is larger than the maternal pelvis, and it cannot descend through the birth canal. Therefore the cesarean section is recommended as the safest mode of delivery for mentum posterior face presentations.
Attempts to manually convert face presentation to vertex, manual or forceps rotation of the persistent posterior chin to anterior are contraindicated as they can be dangerous.
Persistent brow presentation itself is a contraindication for vaginal delivery unless the fetus is significantly small or the maternal pelvis is large.
Continuous electronic fetal heart rate monitoring is recommended for face and brow presentations, as heart rate abnormalities are common in these scenarios. One study found that only 14% of the cases with face presentation had no abnormal traces on the cardiotocograph. [8] It is advised to use external transducer devices to prevent damage to the eyes. When internal monitoring is inevitable, it is suggested to place monitoring devices on bony parts carefully.
People who are usually involved in the delivery of face/ brow presentation are:
- Experienced midwife, preferably looking after laboring woman 1:1
- Senior obstetrician
- Neonatal team - in case of need for resuscitation
- Anesthetic team - to provide necessary pain control (e.g., epidural)
- Theatre team - in case of failure to progress and an emergency cesarean section will be required.
Preparation
No specific preparation is required for face or brow presentation. However, it is essential to discuss the labor options with the mother and birthing partner and inform members of the neonatal, anesthetic, and theatre co-ordinating teams.
Technique or Treatment
Mechanism of Labor in Face Presentation
During contractions, the pressure exerted by the fundus of the uterus on the fetus and pressure of amniotic fluid initiate descent. During this descent, the fetal neck extends instead of flexing. The internal rotation determines the outcome of delivery, if the fetal chin rotates posteriorly, vaginal delivery would not be possible, and cesarean section is permitted. The approach towards mentum-posterior delivery should be individualized, as the cases are rare. Expectant management is acceptable in multiparous women with small fetuses, as a spontaneous mentum-anterior rotation can occur. However, there should be a low threshold for cesarean section in primigravida women or women with large fetuses.
When the fetal chin is rotated towards maternal symphysis pubis as described as mentum-anterior; in these cases further descend through the vaginal canal continues with approximately 73% cases deliver spontaneously. [9] Fetal mentum presses on the maternal symphysis pubis, and the head is delivered by flexion. The occiput is pointing towards the maternal back, and external rotation happens. Shoulders are delivered in the same manner as in vertex delivery.
Mechanism of Labor in Brow Presentation
As this presentation is considered unstable, it is usually converted into a face or an occiput presentation. Due to the cephalic diameter being wider than the maternal pelvis, the fetal head cannot engage; thus, brow delivery cannot take place. Unless the fetus is small or the pelvis is very wide, the prognosis for vaginal delivery is poor. With persistent brow presentation, a cesarean section is required for safe delivery.
Complications
As the cesarean section is becoming a more accessible mode of delivery in malpresentations, the incidence of maternal and fetal morbidity and mortality during face presentation has dropped significantly. [10]
However, there are still some complications associated with the nature of labor in face presentation. Due to the fetal head position, it is more challenging for the head to engage in the birth canal and descend, resulting in prolonged labor.
Prolonged labor itself can provoke foetal distress and arrhythmias. If the labor arrests or signs of fetal distress appear on CTG, the recommended next step in management is an emergency cesarean section, which in itself carries a myriad of operative and post-operative complications.
Finally, due to the nature of the fetal position and prolonged duration of labor in face presentation, neonates develop significant edema of the skull and face. Swelling of the fetal airway may also be present, resulting in respiratory distress after birth and possible intubation.
Clinical Significance
During vertex presentation, the fetal head flexes, bringing the chin to the chest, forming the smallest possible fetal head diameter, measuring approximately 9.5cm. With face and brow presentation, the neck hyperextends, resulting in greater cephalic diameters. As a result, the fetal head will engage later, and labor will progress more slowly. Failure to progress in labor is also more common in both presentations compared to vertex presentation.
Furthermore, when the fetal chin is in a posterior position, this prevents further flexion of the fetal neck, as browns are pressing on the symphysis pubis. As a result, descend through the birth canal is impossible. Such presentation is considered undeliverable vaginally and requires an emergency cesarean section.
Manual attempts to change face presentation to vertex, manual or forceps rotation to mentum anterior are considered dangerous and are discouraged.
Enhancing Healthcare Team Outcomes
A multidisciplinary team of healthcare experts supports the woman and her child during labor and the perinatal period. For a face or brow presentation to be appropriately diagnosed, an experienced midwife and obstetrician must be involved in the vaginal examination and labor monitoring. As fetal anomalies, such as anencephaly or goiter, can contribute to face presentation, sonographers experienced in antenatal scanning should also be involved in the care. It is advised to inform the anesthetic and neonatal teams in advance of the possible need for emergency cesarean section and resuscitation of the neonate. [11] [12]
Gardberg M,Leonova Y,Laakkonen E, Malpresentations--impact on mode of delivery. Acta obstetricia et gynecologica Scandinavica. 2011 May; [PubMed PMID: 21501123]
Tapisiz OL,Aytan H,Altinbas SK,Arman F,Tuncay G,Besli M,Mollamahmutoglu L,Danışman N, Face presentation at term: a forgotten issue. The journal of obstetrics and gynaecology research. 2014 Jun; [PubMed PMID: 24888918]
Zayed F,Amarin Z,Obeidat B,Obeidat N,Alchalabi H,Lataifeh I, Face and brow presentation in northern Jordan, over a decade of experience. Archives of gynecology and obstetrics. 2008 Nov; [PubMed PMID: 18283473]
Bashiri A,Burstein E,Bar-David J,Levy A,Mazor M, Face and brow presentation: independent risk factors. The journal of maternal-fetal [PubMed PMID: 18570114]
Shaffer BL,Cheng YW,Vargas JE,Laros RK Jr,Caughey AB, Face presentation: predictors and delivery route. American journal of obstetrics and gynecology. 2006 May; [PubMed PMID: 16647888]
Bellussi F,Ghi T,Youssef A,Salsi G,Giorgetta F,Parma D,Simonazzi G,Pilu G, The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. American journal of obstetrics and gynecology. 2017 Dec; [PubMed PMID: 28743440]
Ghi T,Eggebø T,Lees C,Kalache K,Rozenberg P,Youssef A,Salomon LJ,Tutschek B, ISUOG Practice Guidelines: intrapartum ultrasound. Ultrasound in obstetrics [PubMed PMID: 29974596]
Benedetti TJ,Lowensohn RI,Truscott AM, Face presentation at term. Obstetrics and gynecology. 1980 Feb; [PubMed PMID: 7352081]
Ducarme G,Ceccaldi PF,Chesnoy V,Robinet G,Gabriel R, [Face presentation: retrospective study of 32 cases at term]. Gynecologie, obstetrique [PubMed PMID: 16630740]
Cruikshank DP,Cruikshank JE, Face and brow presentation: a review. Clinical obstetrics and gynecology. 1981 Jun; [PubMed PMID: 7307363]
Domingues AP,Belo A,Moura P,Vieira DN, Medico-legal litigation in Obstetrics: a characterization analysis of a decade in Portugal. Revista brasileira de ginecologia e obstetricia : revista da Federacao Brasileira das Sociedades de Ginecologia e Obstetricia. 2015 May; [PubMed PMID: 26107576]
. Intrapartum care for healthy women and babies. 2022 Dec 14:(): [PubMed PMID: 32212591]
Use the mouse wheel to zoom in and out, click and drag to pan the image
Brow Presentation
- First Online: 02 August 2023
Cite this chapter

- Syeda Batool Mazhar 2 &
- Zahra Ahmed Muslim 2
534 Accesses
Brow presentation is the rarest of all malpresentations. Anencephaly, neck masses in fetus, polyhydramnios, multiple loops of cord around neck are the fetal factors leading to brow presentation. Contracted pelvis, preterm labour, platypelloid pelvis are some of the contributory maternal factors for brow presentation. Diagnosis is usually made during second stage of labour during prevaginal examination when anterior frontanelle and face are palpated. Cesarean section is performed in brow presentation as it is unusual to get conversion in average sized fetus once membranes have ruptured.
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
- Available as PDF
- Read on any device
- Instant download
- Own it forever
- Available as EPUB and PDF
- Durable hardcover edition
- Dispatched in 3 to 5 business days
- Free shipping worldwide - see info
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
Arulkumaran S, Robson M, editors. Munro Kerr operative obstetrics. 13th ed. Elsevier, Amsterdam; 2019. p. 89–93.
Google Scholar
Malvasi A, Barbera A, Di Vagno G, Gimovsky A, Berghella V, Ghi T, Di Renzo GC, Tinelli A. Asynclitism: a literature review of an often forgotten clinical condition. J Matern Fetal Neonatal Med. 2015;28(16):1890–4. https://doi.org/10.3109/14767058.2014.972925 . Epub 2014 Oct 29.PMID: 25283847.
Article PubMed Google Scholar
Bellussi F, Ghi T, Youssef A, Salsi G, Giorgetta F, Parma D, Simonazzi G, Gianluigi P. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol. 2017;217(6):633–41.
Lanni SM, Gherman R, Gonik B. Malpresentations. Amsterdam: Elsevier; 2017.
Book Google Scholar
Bashiri A, Burstein E, Bar-David J, et al. Face and brow presentation: independent risk factors. J Matern Fetal Neonatal Med. 2008;21(6):357–60.
Hawkins JL, Koffel BL. Chapter 35. In: Chestnut’s obstetric anesthesia: principles and practice: abnormal presentation & multiple gestation. 6th ed; 2020. p. 830.
Meltzer RM, Sactleben MR, Friedman EA. Brow presentation. Obstet Gynecol Surv. 1968;23(6):255–63.
Article Google Scholar
Borell U, Fernstrom I. The mechanism of labour in face and brow presentation: a radiological study. Acta Obstet Gynecol Scand. 1960;39:626–44.
Article CAS PubMed Google Scholar
Levy DL. Persistent brow presentation: a new approach to management. South Med J. 1976;69(2):191–2.
Download references
Author information
Authors and affiliations.
MCH Centre, PIMS, Islamabad, Pakistan
Syeda Batool Mazhar & Zahra Ahmed Muslim
You can also search for this author in PubMed Google Scholar
Editor information
Editors and affiliations.
Department of Obstetrics and Gynecology, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India
Ruchika Garg
Rights and permissions
Reprints and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter
Mazhar, S.B., Muslim, Z.A. (2023). Brow Presentation. In: Garg, R. (eds) Labour and Delivery. Springer, Singapore. https://doi.org/10.1007/978-981-19-6145-8_8
Download citation
DOI : https://doi.org/10.1007/978-981-19-6145-8_8
Published : 02 August 2023
Publisher Name : Springer, Singapore
Print ISBN : 978-981-19-6144-1
Online ISBN : 978-981-19-6145-8
eBook Packages : Medicine Medicine (R0)
Share this chapter
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed, delivery, face and brow presentation, affiliations.
- 1 Vilnius University, Lithuania, Imperial London Healthcare NHS Trust
- 2 University of Health Sciences, Rawalpindi Medical College
- PMID: 33620804
- Bookshelf ID: NBK567727
The term presentation describes the leading part of the fetus or the anatomical structure closest to the maternal pelvic inlet during labor. The presentation can roughly be divided into the following classifications: cephalic, breech, shoulder, and compound. Cephalic presentation is the most common and can be further subclassified as vertex, sinciput, brow, face, and chin. The most common presentation in term labor is the vertex, where the fetal neck is flexed to the chin, minimizing the head circumference.
Face presentation – an abnormal form of cephalic presentation where the presenting part is mentum. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Incidence of face presentation is rare, accounting for approximately 1 in 600 of all presentations.
In brow presentation, the neck is not extended as much as in face presentation, and the leading part is the area between the anterior fontanelle and the orbital ridges. Brow presentation is considered the rarest of all malpresentation with a prevalence of 1 in 500 to 1 in 4000 deliveries.
Both face and brow presentations occur due to extension of the fetal neck instead of flexion; therefore, conditions that would lead to hyperextension or prevent flexion of the fetal neck can all contribute to face or brow presentation. These risk factors may be related to either the mother or the fetus. Maternal risk factors are preterm delivery, contracted maternal pelvis, platypelloid pelvis, multiparity, previous cesarean section, black race. Fetal risk factors include anencephaly, multiple loops of cord around the neck, masses of the neck, macrosomia, polyhydramnios.
These malpresentations are usually diagnosed during the second stage of labor when performing a digital examination. It is possible to palpate orbital ridges, nose, malar eminences, mentum, mouth, gums, and chin in face presentation. Based on the position of the chin, face presentation can be further divided into mentum anterior, posterior, or transverse. In brow presentation, anterior fontanelle and face can be palpated except for the mouth and the chin. Brow presentation can then be further described based on the position of the anterior fontanelle as frontal anterior, posterior, or transverse.
Diagnosing the exact presentation can be challenging, and face presentation may be misdiagnosed as frank breech. To avoid any confusion, a bedside ultrasound scan can be performed. The ultrasound imaging can show a reduced angle between the occiput and the spine or, the chin is separated from the chest. However, ultrasound does not provide much predicting value in the outcome of the labor.
Copyright © 2024, StatPearls Publishing LLC.
PubMed Disclaimer
Conflict of interest statement
Disclosure: Julija Makajeva declares no relevant financial relationships with ineligible companies.
Disclosure: Mohsina Ashraf declares no relevant financial relationships with ineligible companies.
- Continuing Education Activity
- Introduction
- Anatomy and Physiology
- Indications
- Contraindications
- Preparation
- Technique or Treatment
- Complications
- Clinical Significance
- Enhancing Healthcare Team Outcomes
- Review Questions
Similar articles
- Sonographic evaluation of the fetal head position and attitude during labor. Ghi T, Dall'Asta A. Ghi T, et al. Am J Obstet Gynecol. 2022 Jul 6:S0002-9378(22)00449-5. doi: 10.1016/j.ajog.2022.06.003. Online ahead of print. Am J Obstet Gynecol. 2022. PMID: 37278991 Review.
- Sonographic diagnosis of fetal head deflexion and the risk of cesarean delivery. Bellussi F, Livi A, Cataneo I, Salsi G, Lenzi J, Pilu G. Bellussi F, et al. Am J Obstet Gynecol MFM. 2020 Nov;2(4):100217. doi: 10.1016/j.ajogmf.2020.100217. Epub 2020 Aug 18. Am J Obstet Gynecol MFM. 2020. PMID: 33345926
- Leopold Maneuvers. Superville SS, Siccardi MA. Superville SS, et al. 2023 Feb 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. 2023 Feb 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 32809649 Free Books & Documents.
- Stages of Labor. Hutchison J, Mahdy H, Hutchison J. Hutchison J, et al. 2023 Jan 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. 2023 Jan 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 31335010 Free Books & Documents.
- Labor with abnormal presentation and position. Stitely ML, Gherman RB. Stitely ML, et al. Obstet Gynecol Clin North Am. 2005 Jun;32(2):165-79. doi: 10.1016/j.ogc.2004.12.005. Obstet Gynecol Clin North Am. 2005. PMID: 15899353 Review.
- Gardberg M, Leonova Y, Laakkonen E. Malpresentations--impact on mode of delivery. Acta Obstet Gynecol Scand. 2011 May;90(5):540-2. - PubMed
- Tapisiz OL, Aytan H, Altinbas SK, Arman F, Tuncay G, Besli M, Mollamahmutoglu L, Danışman N. Face presentation at term: a forgotten issue. J Obstet Gynaecol Res. 2014 Jun;40(6):1573-7. - PubMed
- Zayed F, Amarin Z, Obeidat B, Obeidat N, Alchalabi H, Lataifeh I. Face and brow presentation in northern Jordan, over a decade of experience. Arch Gynecol Obstet. 2008 Nov;278(5):427-30. - PubMed
- Bashiri A, Burstein E, Bar-David J, Levy A, Mazor M. Face and brow presentation: independent risk factors. J Matern Fetal Neonatal Med. 2008 Jun;21(6):357-60. - PubMed
- Shaffer BL, Cheng YW, Vargas JE, Laros RK, Caughey AB. Face presentation: predictors and delivery route. Am J Obstet Gynecol. 2006 May;194(5):e10-2. - PubMed
Publication types
- Search in PubMed
- Search in MeSH
- Add to Search
Related information
Linkout - more resources, full text sources.
- NCBI Bookshelf

- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.

- 2022 New Pearls of Exxcellence Articles
Management of Brow, Face, and Compound Malpresentations
Author: Meera Kesavan, MD
Mentor: Lisa Keder MD Editor: Daniel JS Martingano DO MBA PhD
Registered users can also download a PDF or listen to a podcast of this Pearl. Log in now , or create a free account to access bonus Pearls features.
Fetal malpresentation, including brow, face, or compound presentations, complicates around 3-4% of all term births. Because these abnormal fetal presentations still are cephalic, many such cases result in vaginal deliveries, yet there are increased risks for adverse outcomes, including cesarean delivery resultant surgical complications, persistent malpresentation precluding vaginal delivery, and abnormal labor resulting in arrest of dilation or descent.
These fetal malpresentation are differentiated in the following ways:
- In face presentations, the presenting part is the mentum, which is further divided based on its position, including mentum posterior, mentum transverse or mentum anterior positions. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Mentum anterior malpresentations can potentially achieve vaginal deliveries, whereas mentum posterior malpresentations cannot.
- In brow presentations, there is less extension of the fetal neck as in face presentations making the leading fetal part being the area between the anterior fontanelle and the orbital ridges. These presentations are uncommon and are managed similarly to face presentations. Brow presentation can be further described based on the position of the anterior fontanelle as frontal anterior, posterior, or transverse.
- Compound presentation is defined as the leading fetal part, including a fetal extremity, alongside a cephalic or breech presentation. Management of compound presentations is expected (and often incidentally noted following delivery) because the extremity will often either retract as the head descends or will feasibly allow for delivery in its current position, with manipulation attempts to reduce the compound presentation usually avoided.
Risk factors for brow and face presentations include fetal CNS malformations, congenital or chromosomal anomalies, advanced maternal age, low birthweight, abnormal maternal pelvic anatomy (e.g. contracted pelvis, cephalopelvic disporotion, platypelloid pelvis, etc.) and nulliparity. non-Hispanic White women have the highest risk for malpresentation, whereas non-Hispanic Black women have the lowest risk.
Diagnosis usually is made during the second stage of labor while performing routine vaingla examinations and involves palpation of the abnormal leading fetal part (forehead, orbital ridge, orbits, nose, etc.) Obstetric ultrasound can additionally provide complimentary information to support these diagnoses and distinguish from other fetal malpresentations or malpositions. In face presentation, the mentum (chin) and mouth are palpable.
Management considerations for face, brow, and compounds presentations are unique with compound presentations having higher rates of vaginal delivery and lower complications as compared to either brow or face presentations.
- For brow presentations, approximately 30-40% of brow presentations will convert to a face presentation, and about 20% will convert to a vertex presentation. Anterior positions have the possibility of vaginal deliveries and can be managed by usual labor management principles, whereas mentum posterior positions are indications for cesarean delivery.
- For face presentations, the likelihood of vaginal delivery depends on the orientation of the mentum, with mentum anterior being most suitable for vaginal delivery. If the fetus is mentum posterior, flexion of the neck is precluded and results in the inability of fetal descent.
- For compound presentations, management is expectant and manipulation of the leading extremities should be avoided. Most cases of compound presentation result in vaginal deliveries. For term deliveries, compound presentations with parts other than the hand are unlikely to result in safe vaginal delivery.
Labor management for brow and face presentation overall involves continuous fetal heart rate monitoring and repeat clinical assessments, given the increased potential of fetal complications as noted. Caution should be used with internal monitoring devices, which can cause ophthalmic injury or trauma to the presenting fetal parts, with the use of fetal scalp electrodes discouraged and intrauterine pressure catheters acceptable with appropriate clinical judgment and feasibility.
Midforceps, breech extraction, and manual manipulation are not recommended and increase the risk of maternal and neonatal morbidity.
Neonatal outcomes for both face and brow presentations include facial edema, bruising, and soft tissue trauma. Complications of compound presentation specifically include umbilical cord prolapse and injury to the presenting limb. With appropriate management, neonatal and maternal morbidity for face, brow, and compound presentations are low.
Further Reading:
Bar-El L, Eliner Y, Grunebaum A, Lenchner E, et al. Race and ethnicity are among the predisposing factors for fetal malpresentation at term. Am J Obstet Gynecol MFM. 2021 Sep;3(5):100405. doi: 10.1016/j.ajogmf.2021.100405. Epub 2021 Jun 4. PMID: 34091061.
Bellussi F, Ghi T, Youssef A, et al. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol. 2017 Dec;217(6):633-641. doi: 10.1016/j.ajog.2017.07.025. Epub 2017 Jul 22. PMID: 28743440 .
Pilliod RA, Caughey AB. Fetal Malpresentation and Malposition: Diagnosis and Management. Obstet Gynecol Clin North Am. 2017 Dec;44(4):631-643. doi: 10.1016/j.ogc.2017.08.003. PMID: 29078945 .
Zayed F, Amarin Z, Obeidat B, et al. Face and brow presentation in northern Jordan, over a decade of experience. Arch Gynecol Obstet. 2008 Nov;278(5):427-30. doi: 10.1007/s00404-008-0600-0. Epub 2008 Feb 19. PMID: 18283473 .
Initial Approval: August 2013; Revised: 11/2016; Revised July 2018; Reaffirmed January 2020; Revised September 2021. Revised July 2023.
This site uses cookies.

This feature is only available for registered users.
Log in here:, not a registered user.
Becoming a registered user gives you access to special features like PDF downloads and podcast episodes of each SASGOG Pearl of Exxcellence.
Create a Free Account
Are you sure you want to remove this Pearl from your favorites list?
- GP practice services
- Health advice
- Health research
- Medical professionals
Health topics
Advice and clinical information on a wide variety of healthcare topics.
All health topics
Latest features
Allergies, blood & immune system
Bones, joints and muscles
Brain and nerves
Chest and lungs
Children's health
Cosmetic surgery
Digestive health
Ear, nose and throat
General health & lifestyle
Heart health and blood vessels
Kidney & urinary tract
Men's health
Mental health
Oral and dental care
Senior health
Sexual health
Signs and symptoms
Skin, nail and hair health
Travel and vaccinations
Treatment and medication
Women's health
Healthy living
Expert insight and opinion on nutrition, physical and mental health.
Exercise and physical activity
Healthy eating
Healthy relationships
Managing harmful habits
Mental wellbeing
Relaxation and sleep
Managing conditions
From ACE inhibitors for high blood pressure, to steroids for eczema, find out what options are available, how they work and the possible side effects.
Featured conditions
ADHD in children
Crohn's disease
Endometriosis
Fibromyalgia
Gastroenteritis
Irritable bowel syndrome
Polycystic ovary syndrome
Scarlet fever
Tonsillitis
Vaginal thrush
Health conditions A-Z
Medicine information
Information and fact sheets for patients and professionals. Find out side effects, medicine names, dosages and uses.
All medicines A-Z
Allergy medicines
Analgesics and pain medication
Anti-inflammatory medicines
Breathing treatment and respiratory care
Cancer treatment and drugs
Contraceptive medicines
Diabetes medicines
ENT and mouth care
Eye care medicine
Gastrointestinal treatment
Genitourinary medicine
Heart disease treatment and prevention
Hormonal imbalance treatment
Hormone deficiency treatment
Immunosuppressive drugs
Infection treatment medicine
Kidney conditions treatments
Muscle, bone and joint pain treatment
Nausea medicine and vomiting treatment
Nervous system drugs
Reproductive health
Skin conditions treatments
Substance abuse treatment
Vaccines and immunisation
Vitamin and mineral supplements
Tests & investigations
Information and guidance about tests and an easy, fast and accurate symptom checker.
About tests & investigations
Symptom checker
Blood tests
BMI calculator
Pregnancy due date calculator
General signs and symptoms
Patient health questionnaire
Generalised anxiety disorder assessment
Medical professional hub
Information and tools written by clinicians for medical professionals, and training resources provided by FourteenFish.
Content for medical professionals
FourteenFish training
- Professional articles
Evidence-based professional reference pages authored by our clinical team for the use of medical professionals.
View all professional articles A-Z
Actinic keratosis
Bronchiolitis
Molluscum contagiosum
Obesity in adults
Osmolality, osmolarity, and fluid homeostasis
Recurrent abdominal pain in children
Medical tools and resources
Clinical tools for medical professional use.
All medical tools and resources
Malpresentations and malpositions
Peer reviewed by Dr Laurence Knott Last updated by Dr Colin Tidy, MRCGP Last updated 22 Jun 2021
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find one of our health articles more useful.
In this article :
Malpresentation, malposition.
Usually the fetal head engages in the occipito-anterior position (more often left occipito-anterior (LOA) rather than right) and then undergoes a short rotation to be directly occipito-anterior in the mid-cavity. Malpositions are abnormal positions of the vertex of the fetal head relative to the maternal pelvis. Malpresentations are all presentations of the fetus other than vertex.
Obstetrics - the pelvis and head

Continue reading below
Predisposing factors to malpresentation include:
Prematurity.
Multiple pregnancy.
Abnormalities of the uterus - eg, fibroids.
Partial septate uterus.
Abnormal fetus.
Placenta praevia.
Primiparity.
Breech presentation
See the separate Breech Presentations article for more detailed discussion.
Breech presentation is the most common malpresentation, with the majority discovered before labour. Breech presentation is much more common in premature labour.
Approximately one third are diagnosed during labour when the fetus can be directly palpated through the cervix.
After 37 weeks, external cephalic version can be attempted whereby an attempt is made to turn the baby manually by manipulating the pregnant mother's abdomen. This reduces the risk of non-cephalic delivery 1 .
Maternal postural techniques have also been tried but there is insufficient evidence to support these 2 .
Many women who have a breech presentation can deliver vaginally. Factors which make this less likely to be successful include 3 :
Hyperextended neck on ultrasound.
High estimated fetal weight (more than 3.8 kg).
Low estimated weight (less than tenth centile).
Footling presentation.
Evidence of antenatal fetal compromise.
Transverse lie 4
When the fetus is positioned with the head on one side of the pelvis and the buttocks in the other (transverse lie), vaginal delivery is impossible.
This requires caesarean section unless it converts or is converted late in pregnancy. The surgeon may be able to rotate the fetus through the wall of the uterus once the abdominal wall has been opened. Otherwise, a transverse uterine incision is needed to gain access to a fetal pole.
Internal podalic version is no longer attempted.
Transverse lie is associated with a risk of cord prolapse of up to 20%.
Occipito-posterior position
This is the most common malposition where the head initially engages normally but then the occiput rotates posteriorly rather than anteriorly. 5.2% of deliveries are persistent occipito-posterior 5 .
The occipito-posterior position results from a poorly flexed vertex. The anterior fontanelle (four radiating sutures) is felt anteriorly. The posterior fontanelle (three radiating sutures) may also be palpable posteriorly.
It may occur because of a flat sacrum, poorly flexed head or weak uterine contractions which may not push the head down into the pelvis with sufficient strength to produce correct rotation.
As occipito-posterior-position pregnancies often result in a long labour, close maternal and fetal monitoring are required. An epidural is often recommended and it is essential that adequate fluids be given to the mother.
The mother may get the urge to push before full dilatation but this must be discouraged. If the head comes into a face-to-pubis position then vaginal delivery is possible as long as there is a reasonable pelvic size. Otherwise, forceps or caesarean section may be required.
Occipito-transverse position
The head initially engages correctly but fails to rotate and remains in a transverse position.
Alternatives for delivery include manual rotation of fetal head using Kielland's forceps, or delivery using vacuum extraction. This is inappropriate if there is any fetal acidosis because of the risk of cerebral haemorrhage.
Therefore, there must be provision for a failure of forceps delivery to be changed immediately to a caesarean. The trial of forceps is therefore often performed in theatre. Some centres prefer to manage by caesarean section without trial of forceps.
Face presentations
Face presents for delivery if there is complete extension of the fetal head.
Face presentation occurs in 1 in 1,000 deliveries 5 .
With adequate pelvic size, and rotation of the head to the mento-anterior position, vaginal delivery should be achieved after a long labour.
Backwards rotation of the head to a mento-posterior position requires a caesarean section.
Brow positions
The fetal head stays between full extension and full flexion so that the biggest diameter (the mento-vertex) presents.
Brow presentation occurs in 0.14% of deliveries 5 .
Brow presentation is usually only diagnosed once labour is well established.
The anterior fontanelle and super orbital ridges are palpable on vaginal examination.
Unless the head flexes, a vaginal delivery is not possible, and a caesarean section is required.
Further reading and references
- Hofmeyr GJ, Kulier R, West HM ; External cephalic version for breech presentation at term. Cochrane Database Syst Rev. 2015 Apr 1;(4):CD000083. doi: 10.1002/14651858.CD000083.pub3.
- Hofmeyr GJ, Kulier R ; Cephalic version by postural management for breech presentation. Cochrane Database Syst Rev. 2012 Oct 17;10:CD000051. doi: 10.1002/14651858.CD000051.pub2.
- Management of Breech Presentation ; Royal College of Obstetricians and Gynaecologists (Mar 2017)
- Szaboova R, Sankaran S, Harding K, et al ; PLD.23 Management of transverse and unstable lie at term. Arch Dis Child Fetal Neonatal Ed. 2014 Jun;99 Suppl 1:A112-3. doi: 10.1136/archdischild-2014-306576.324.
- Gardberg M, Leonova Y, Laakkonen E ; Malpresentations - impact on mode of delivery. Acta Obstet Gynecol Scand. 2011 May;90(5):540-2. doi: 10.1111/j.1600-0412.2011.01105.x.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 21 Jun 2026
22 jun 2021 | latest version.
Last updated by
Peer reviewed by

Feeling unwell?
Assess your symptoms online for free
Uptodate Reference Title
Face and brow presentations in labor.
INTRODUCTION — The vast majority of fetuses at term are in cephalic presentation. Approximately 5 percent of these fetuses are in a cephalic malpresentation, such as occiput posterior or transverse, face ( figure 1A-B ), or brow ( figure 2 ) [ 1 ].
Diagnosis and management of face and brow presentations will be reviewed here. Other cephalic malpresentations are discussed separately. (See "Occiput posterior position" and "Occiput transverse position" .)
Prevalence — Face and brow presentation are uncommon. Their prevalences compared with other types of malpresentations are shown below [ 1-9 ]:
● Occiput posterior – 1/19 deliveries
● Breech – 1/33 deliveries
● Face – 1/600 to 1/800 deliveries
● Brow – 1/500 to 1/4000 deliveries
● Transverse lie – 1/833 deliveries
● Compound – 1/1500 deliveries
The prevalence of face presentation at Parkland Memorial Hospital in Texas (United States) has decreased to 1/2000 deliveries in recent years [ 10 ], possibly because of fewer deliveries of fetuses with anomalies such as anencephaly [ 11,12 ]; however, others have not observed a decline [ 9,12,13 ].
Clinical significance — During labor in the occiput anterior presentation, the neck normally flexes to bring the chin to the chest, resulting in the relatively small suboccipito-bregmatic diameter (average length 9.5 cm) as the widest cephalic diameter that needs to negotiate the pelvis. This diameter is generally able to traverse the obstetric conjugate (average length 10.5 cm) ( figure 3 ), which is the shortest anteroposterior pelvic diameter. By comparison, the neck is extended in brow and face presentations, which present larger fetal cephalic diameters that need to negotiate the pelvis ( figure 4 ). Thus, protraction or arrest of descent is more likely, which increases the chances of maternal and neonatal morbidity from vaginal birth and the frequency for cesarean birth. Brow and mentum posterior face presentations are most likely to exhibit cephalopelvic dystocia unless the fetus is very small or the maternal pelvis is very large or both. (See 'Neonatal outcome' below and 'Neonatal outcome' below.)
Fetal heart rate abnormalities are more common than with occiput anterior position [ 2,14 ]. They may be due to more head compression or a higher frequency of cord compression.
Risk factors — Maternal or fetal anatomic factors that prevent flexion or favor extension of the fetal neck increase the risk for face/brow presentation. These factors include anencephaly, severe hydrocephalus with cephalomegaly, anterior neck mass, multiple nuchal cords, cephalopelvic disproportion, preterm birth/low birth weight, macrosomia, contracted maternal pelvis, platypelloid pelvis ( figure 5 ), multiparity, polyhydramnios, previous cesarean birth, and Black race [ 2,5,8,9,11-13 ].
In multiparous patients, poor abdominal muscle tone may permit the uterine fundus and fetal trunk to swing anteriorly, which may extend the cervical spine, leading to a face or brow presentation [ 13 ]. Alternatively, late engagement of the vertex in multiparous patients, often after the onset of labor, may be the predisposing factor [ 12 ].
A contracted maternal pelvis predisposes to malpresentation [ 12 ]. The increased risk of face/brow presentation in Black patients may be due to differences in pelvic dimensions between White and Black females and a higher rate of preterm birth in Black individuals [ 13,15-17 ]. The differences in pelvic dimensions may be related to environmental differences (eg, locomotion, load carrying, health, nutrition) [ 18 ].
Although preterm birth has been linked to face/brow presentation, possibly because a very small fetus can descend with the neck partially extended, the association between preterm birth and face presentation is weak [ 9,13 ].
Pregnancies with polyhydramnios may be at risk secondary to impaired swallowing due to a fetal anomaly (particularly anencephaly) [ 12 ] or to obstruction of the fetal trachea and esophagus from a hyperextended fetal neck [ 5 ].
FACE PRESENTATION
Definition — Face presentation refers to a fetal presentation in which the fetal face from forehead to chin is the leading fetal body part descending into the birth canal ( figure 1B ). The fetal neck is highly extended (sharply deflexed), such that the occiput may touch the back.
Diagnosis — The intrapartum diagnosis of face presentation is made by vaginal examination in the late first or the second stage of labor [ 5 ]. Palpation of the orbital ridge and orbits, saddle of the nose, mouth, and chin is diagnostic of face presentation. The fontanelles and sutures are not generally palpable [ 19 ]. At diagnosis, nearly 60 percent of face presentations are mentum anterior, 26 percent are mentum posterior, and 15 percent are mentum transverse, and may be designated as left or right ( figure 1A ) [ 11 ].
Intrapartum transabdominal, translabial, and/or transvaginal sonography of a face presentation will show a hyperextended fetal neck, with the orbits and nasal bridge at the center of the presenting part in the mid-sagittal plane [ 20 ]. Although imaging studies can be performed to confirm the diagnosis if it is uncertain, imaging is not mandatory, and results do not have prognostic value for predicting the outcome of labor [ 21 ].
Differential diagnosis — Face presentation may be misdiagnosed as a frank breech presentation on digital examination since the latter is more commonly encountered (and therefore expected). Both presentations are characterized by soft tissues with an orifice; however, careful palpation will identify the bony facial structures and lead to the correct diagnosis. With ultrasound readily available in most delivery units, confirmation of the type of malpresentation (breech or face) is easily obtained if needed.
Labor and delivery management
Fetal heart rate monitoring — The fetal heart rate is monitored continuously, ideally with an external device. An internal device may cause facial or ophthalmic injuries if improperly placed [ 22-24 ]. If internal monitoring is required, the electrode should be carefully applied over a bony structure such as the forehead, mandible, or zygomatic bones to minimize the risk of trauma [ 25 ].
Abnormalities of the fetal heart rate occur more frequently with face presentations [ 4,25,26 ]. In one series, severe variable and late decelerations developed in 29 and 24 percent of labors, respectively [ 25 ]. Only 14 percent of pregnancies had normal tracings. Moreover, 13 percent of the newborns had a low five-minute Apgar score.
Interpretation and management of abnormal fetal heart rate tracings are not affected by fetal presentation and are reviewed separately. We perform amnioinfusion for patients with variable decelerations (category 2 tracing), regardless of presentation, as long as vaginal birth is anticipated. (See "Intrapartum category I, II, and III fetal heart rate tracings: Management" .)
Mentum anterior — In mentum anterior face presentation, the fetal chin needs to pass under the symphysis pubis. For this to occur, the extended fetal neck may need to extend even more. After the chin clears the symphysis, further descent and fetal expulsion can occur [ 5 ]. Over 75 percent of mentum anterior fetuses are born vaginally [ 2,3,13,26,27 ].
The parturient may begin pushing at full dilation. Labor progress should be closely monitored as arrest of descent may occur, although not inevitably as in persistent mentum posterior position.
Oxytocin augmentation and cesarean birth are performed for standard obstetric indications [ 26 ]. (See "Labor: Overview of normal and abnormal progression" .)
Attempts at version or vacuum- or midforceps-assisted delivery should be avoided as they are associated with unnecessary maternal trauma and neonatal injury [ 28 ].
An outlet forceps-assisted delivery when the face is distending the perineum is not contraindicated if delivery must be facilitated but should only be performed by experienced clinicians familiar with the particular considerations involved. For example, in contrast to the occiput anterior position, engagement does not occur until the face is at +2 station [ 5 ]; the chin rather than the occiput is the focal point for orientation; and if Kielland forceps are applied, the left blade is applied to the right side of the head and the right blade to the left side [ 29,30 ]. The technique of forceps delivery is beyond the scope of this review.
Mentum posterior — In the mentum posterior face presentation, the fetal neck is already maximally extended and cannot extend further to allow the occiput to pass under the symphysis. Therefore, the mentum posterior face presentation will not deliver vaginally unless spontaneous rotation to mentum anterior occurs ( figure 6 ), often late in the second stage of labor [ 14 ], or the fetus is very small, or the pelvis is very large. If the fetal status is reassuring and there is normal labor progress, mentum posterior presentation can be managed expectantly to see if spontaneous rotation will occur [ 14 ].
Patients with abnormal labor progression are delivered by cesarean. We individualize management when labor is progressing. For example, in multiparous patients with an adequate pelvis and fetus estimated to weigh less than their prior newborns, we would follow labor progress closely and maintain a low threshold for abandoning attempts at vaginal birth if labor does not progress normally in the first or second stage. However, if the fetus is estimated to be larger than their prior newborns, or in nulliparous patients, we would recommend cesarean birth early in the labor course. There is consensus that assisted vaginal delivery is contraindicated for mentum posterior presentations [ 14,31,32 ].
In the past, manual version of the mentum posterior face to an occiput anterior or mentum anterior position was attempted using internal and external manipulation [ 33,34 ]. Although some clinicians have been successful with no serious neonatal or maternal complications, others have reported maternal deaths from uterine rupture, cord prolapse resulting in neonatal asphyxia, and cervical spine trauma resulting in severe neonatal neurologic sequelae [ 28 ]. Given the safety and ready availability of cesarean birth, we believe internal version should be reserved for occasions when cesarean birth is unable to be accomplished due to lack of surgical facilities and inability to arrange maternal transport, or absolute maternal refusal to allow a cesarean birth [ 34 ].
Mentum transverse — There are minimal published data on management of the mentum transverse position. Our management is the same as for mentum posterior.
Neonatal outcome — Prior to 1955, increased rates of intrapartum fetal death and perinatal mortality (approximately 10 percent) were reported for face presentation [ 5 ]. Perinatal mortality decreased to 2 to 3 percent by 1980, likely due to the increased use of cesarean birth, as well as other advances in obstetric and neonatal care [ 5 ]. Recent perinatal mortality data are not available.
Neonates who were in face presentation often have significant facial edema, facial bruising/ecchymosis, and skull molding [ 35 ]. This usually resolves within the first 24 to 48 hours of life. Personnel and equipment for performing endotracheal intubation should be readily available at birth [ 25 ]. Difficulty in ventilation during resuscitation has been reported and attributed to tracheal and laryngeal trauma and edema.
Facial trauma and spinal cord injury have also been described in case reports and are often associated with version, extraction, and midforceps rotations [ 2,23-25,36 ]. Appropriate management of face presentation, as described above, typically does not result in increased serious maternal or neonatal morbidity [ 2 ].
BROW PRESENTATION
Definition — Brow presentation refers to a presentation in which the fetal surface presenting in the birth canal extends from the anterior fontanelle to the brow (orbital ridge), but does not include the mouth and chin ( figure 2 ). The fetal neck is extended, but not to the degree of a face presentation.
Diagnosis — The diagnosis of brow presentation is made by vaginal examination in the second stage of labor [ 5 ]. Palpation of the forehead, orbital ridge, orbits, and saddle of the nose, but not the mouth and chin, is diagnostic of brow presentation. The anterior fontanelle is palpable, but the sagittal suture generally is not [ 19 ]. The brow may be anterior or posterior and described by the position or the anterior fontanelle as frontal anterior, transverse, or posterior [ 14 ].
There is increasing evidence that ultrasound is more accurate than vaginal examination for determining fetal position and can be used to determine or confirm abnormal presentation [ 37,38 ]. On transabdominal examination, if the occiput is anterior, the main finding is a reduction in occiput-spinal angle, usually around 90 degrees rather than over 120 degrees; if the occiput is posterior, the chin is separate from chest, and the cervical spine is curved (convex) anteriorly [ 19 ]. If a transperineal examination is performed, the fetal orbits are seen at the same level as the pubic symphysis.
Labor and delivery management — The fetal heart rate is monitored continuously during labor, ideally with an external device, since fetal heart rate abnormalities are more common than with occiput anterior position. An internal device may cause facial or ophthalmic injuries if improperly placed [ 22-24 ]. If internal monitoring is required, the electrode should be cautiously applied over a bony structure, such as the forehead, to minimize the risk of trauma [ 25 ].
Patients with a clinically adequate or proven pelvis can undergo a trial of labor since many brow presentations are transitional. In one review, when brow presentation was diagnosed early in labor, 67 to 75 percent of fetuses spontaneously converted to a more favorable presentation and delivered vaginally. When diagnosed late in labor, 50 percent spontaneously converted and delivered vaginally: in 30 percent, the neck extended further resulting in mentum anterior face presentation; in 20 percent, the neck flexed resulting in an occiput posterior presentation [ 2,5,39 ]. Conversion to occiput anterior is rare.
If the brow presentation persists, labor progress is usually protracted or arrests, necessitating cesarean birth. Oxytocin augmentation is not recommended in this setting, given the association between brow presentation and cephalopelvic disproportion [ 5,26,33 ]. Version or vacuum- or forceps-assisted delivery are not recommended, as the risks for maternal and fetal injury are high [ 5,14,31,32 ]. However, in settings where cesarean birth is not readily available, vacuum-assisted flexion of the fetal head may be considered [ 40 ].
In a minority of cases, spontaneous vaginal birth may be possible if the fetus is extremely small or macerated or the maternal pelvis is unusually large.
Neonatal outcome — Recognition and appropriate management of brow presentation, as described above, typically do not result in increased serious maternal or neonatal morbidity.
SOCIETY GUIDELINE LINKS — Links to society and government-sponsored guidelines from selected countries and regions around the world are provided separately. (See "Society guideline links: Labor" .)
SUMMARY AND RECOMMENDATIONS
Issues common to face and brow presentations
● Risk factors – Face and brow presentations are associated with multiparity, cephalopelvic disproportion, preterm birth, polyhydramnios, and fetal anomalies (eg, anencephaly, anterior neck mass). (See 'Risk factors' above.)
● Clinical significance – The deflexed neck in face or brow presentation inhibits head engagement and subsequent fetal descent. (See 'Clinical significance' above.)
● Cautions – The fetal heart rate is monitored continuously during labor, ideally with an external device, because of the increased prevalence of fetal heart rate decelerations. An internal device may cause facial or ophthalmic injuries if improperly placed. If internal monitoring is required, the electrode should be carefully applied over a bony structure to minimize the risk of trauma. (See 'Labor and delivery management' above.)
● Definition – In face presentation, the fetal face from forehead to chin is the leading fetal body part descending into the birth canal ( figure 1B ). The fetal neck is sharply deflexed and the occiput may touch the back. Nearly 60 percent of face presentations are mentum anterior, 26 percent are mentum posterior, and 15 percent are mentum transverse, and may be designated as left or right ( figure 1A ). (See 'Definition' above.)
● Diagnosis – The diagnosis of face presentation is made by vaginal examination. Palpation of the orbital ridge and orbits, saddle of the nose, mouth, and chin is diagnostic of face presentation ( figure 1A ). Ultrasound can be used to confirm or clarify the type of malpresentation if the clinical examination findings are unclear. (See 'Diagnosis' above.)
● Management
• Mentum anterior – Over 75 percent of mentum anterior fetuses deliver vaginally; this rate is similar to that for all fetuses in cephalic presentations. For face presentation with the mentum anterior, we suggest a trial of labor rather than cesarean birth ( Grade 2C ). Oxytocin augmentation may be administered in the setting of a normal fetus with protracted labor, as long as the fetal heart rate pattern remains reassuring. (See 'Labor and delivery management' above.)
• Mentum posterior – The mentum posterior face presentation will not deliver vaginally unless spontaneous rotation occurs, which is infrequent and occurs late in the second stage of labor, or the fetus is very small or the pelvis very large or both. As mentum posterior presentations are rare, we individualize management of such situations. In a multiparous patient with an adequate pelvis and fetus estimated to weigh less than her prior newborns, we follow labor progress closely and maintain a low threshold for abandoning attempts at vaginal birth if labor does not progress normally in the first or second stage. We recommend cesarean birth rather than manual rotation ( Grade 1C ).
If the fetus is estimated to be larger than the patient’s prior newborns or the patient is nulliparous, we perform cesarean birth early in the labor course. (See 'Labor and delivery management' above.)
● Definition – In brow presentation, the fetal surface presenting in the birth canal extends from the anterior fontanelle to the brow (orbital ridge), but does not include the mouth and chin ( figure 2 ). The fetal neck is extended, but not to the degree of a face presentation. (See 'Definition' above.)
● Diagnosis – The diagnosis of brow presentation is made by vaginal examination. Palpation of the forehead, orbital ridge, orbits, and saddle of the nose, but not the mouth and chin, is diagnostic of brow presentation ( figure 2 ). Ultrasound can be used to confirm or clarify the type of malpresentation if the clinical examination findings are unclear. (See 'Diagnosis' above.)
● Management – Patients with a fetus in brow presentation and a clinically adequate or proven pelvis can undergo a trial of labor, with close monitoring and delivery by cesarean for standard indications. The brow presentation is often a transitional state: 50 percent will spontaneously convert to a face or occipital presentation. Fetuses with persistent brow presentation should be delivered by cesarean since vaginal birth is not possible unless the fetus is very small, the pelvis is very large, or both. Operative vaginal delivery is contraindicated for brow presentation. (See 'Labor and delivery management' above.)
ACKNOWLEDGMENT — The UpToDate editorial staff acknowledges Svena Julien, MD, who contributed to earlier versions of this topic review.
- Gardberg M, Leonova Y, Laakkonen E. Malpresentations--impact on mode of delivery. Acta Obstet Gynecol Scand 2011; 90:540.
- Duff P. Diagnosis and management of face presentation. Obstet Gynecol 1981; 57:105.
- Ducarme G, Ceccaldi PF, Chesnoy V, et al. [Face presentation: retrospective study of 32 cases at term]. Gynecol Obstet Fertil 2006; 34:393.
- Bhal PS, Davies NJ, Chung T. A population study of face and brow presentation. J Obstet Gynaecol 1998; 18:231.
- Cruikshank DP, Cruikshank JE. Face and brow presentation: a review. Clin Obstet Gynecol 1981; 24:333.
- Weissberg SM, O'Leary JA. Compound presentation of the fetus. Obstet Gynecol 1973; 41:60.
- Ingólfsson A. Brow presentations. Acta Obstet Gynecol Scand 1969; 48:486.
- Tapisiz OL, Aytan H, Altinbas SK, et al. Face presentation at term: a forgotten issue. J Obstet Gynaecol Res 2014; 40:1573.
- Zayed F, Amarin Z, Obeidat B, et al. Face and brow presentation in northern Jordan, over a decade of experience. Arch Gynecol Obstet 2008; 278:427.
- Cunningham FG, Leveno KJ, Bloom SL, et al. Williams Obstetrics, 25th ed, McGraw-Hill Education, New York 2018.
- Cruikshank DP, White CA. Obstetric malpresentations: twenty years' experience. Am J Obstet Gynecol 1973; 116:1097.
- Bashiri A, Burstein E, Bar-David J, et al. Face and brow presentation: independent risk factors. J Matern Fetal Neonatal Med 2008; 21:357.
- Shaffer BL, Cheng YW, Vargas JE, et al. Face presentation: predictors and delivery route. Am J Obstet Gynecol 2006; 194:e10.
- Sharshiner R, Silver RM. Management of fetal malpresentation. Clin Obstet Gynecol 2015; 58:246.
- Handa VL, Lockhart ME, Fielding JR, et al. Racial differences in pelvic anatomy by magnetic resonance imaging. Obstet Gynecol 2008; 111:914.
- Işcan MY. Assessment of race from the pelvis. Am J Phys Anthropol 1983; 62:205.
- Patriquin ML, Steyn M, Loth SR. Metric analysis of sex differences in South African black and white pelves. Forensic Sci Int 2005; 147:119.
- Kurki HK, Decrausaz SL. Shape variation in the human pelvis and limb skeleton: Implications for obstetric adaptation. Am J Phys Anthropol 2016; 159:630.
- Bellussi F, Ghi T, Youssef A, et al. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol 2017; 217:633.
- Lau WL, Cho LY, Leung WC. Intrapartum translabial ultrasound demonstration of face presentation during first stage of labor. J Obstet Gynaecol Res 2011; 37:1868.
- Ghi T, Eggebø T, Lees C, et al. ISUOG Practice Guidelines: intrapartum ultrasound. Ultrasound Obstet Gynecol 2018; 52:128.
- Lauer AK, Rimmer SO. Eyelid laceration in a neonate by fetal monitoring spiral electrode. Am J Ophthalmol 1998; 125:715.
- Miyashiro MJ, Mintz-Hittner HA. Penetrating ocular injury with a fetal scalp monitoring spiral electrode. Am J Ophthalmol 1999; 128:526.
- Cheng BT, Laurenti KD, Kurup SP. Neonatal eyelid penetration from insertion of a fetal scalp electrode: a case report. BMC Pregnancy Childbirth 2022; 22:878.
- Benedetti TJ, Lowensohn RI, Truscott AM. Face presentation at term. Obstet Gynecol 1980; 55:199.
- Schwartz Z, Dgani R, Lancet M, Kessler I. Face presentation. Aust N Z J Obstet Gynaecol 1986; 26:172.
- Westgren M, Svenningsen NW. Face presentation in modern obstetrics--a study with special reference to fetal long term morbidity. Z Geburtshilfe Perinatol 1984; 188:87.
- Vialle R, Piétin-Vialle C, Ilharreborde B, et al. Spinal cord injuries at birth: a multicenter review of nine cases. J Matern Fetal Neonatal Med 2007; 20:435.
- Dennen PC. Dennen's Forceps Deliveries, 3rd edition, FA Davis, Philadelphia 1989. p.127.
- Laufe LE. Obstetric Forceps, Harper & Row, Hagerstown 1968. p.117.
- Yeomans ER, Hoffman BL, Gilstrap LC, Cunningham FG. Operative vaginal delivery. In: Cunningham and Gilstrap's Operative Obstetrics, 3rd ed, McGraw-Hill Education, New York 2017.
- Shabib G, Black, A. Operative vaginal delivery. In: Oxorn-Foote Human Labor and Birth, 6th ed, Posner G (Ed), McGraw-Hill Medical, New York 2013.
- Levy DL. Persistent brow presentation: a new approach to management. South Med J 1976; 69:191.
- Neuman M, Beller U, Lavie O, et al. Intrapartum bimanual tocolytic-assisted reversal of face presentation: preliminary report. Obstet Gynecol 1994; 84:146.
- Williams Obstetrics, 23rd Ed, Cunningham, FG, Leveno, KJ, Bloom, JC, et al (Eds), McGraw-Hill, 2010.
- Vialle R, Piétin-Vialle C, Vinchon M, et al. Birth-related spinal cord injuries: a multicentric review of nine cases. Childs Nerv Syst 2008; 24:79.
- Lau WL, Leung WC, Chin R. Intrapartum translabial ultrasound demonstrating brow presentation during the second stage of labor. Int J Gynaecol Obstet 2009; 107:62.
- Wiafe YA, Whitehead B, Venables H, Nakua EK. The effectiveness of intrapartum ultrasonography in assessing cervical dilatation, head station and position: A systematic review and meta-analysis. Ultrasound 2016; 24:222.
- Jennings PN. Brow presentation with vaginal delivery. Aust N Z J Obstet Gynaecol 1968; 8:219.
- Luker R. Vaginal delivery of two cases of brow presentation using multiple Kiwi Omnicups. J Obstet Gynaecol 2005; 25:601.
1 : Malpresentations--impact on mode of delivery.
2 : Diagnosis and management of face presentation.
3 : [Face presentation: retrospective study of 32 cases at term].
4 : A population study of face and brow presentation.
5 : Face and brow presentation: a review.
6 : Compound presentation of the fetus.
7 : Brow presentations.
8 : Face presentation at term: a forgotten issue.
9 : Face and brow presentation in northern Jordan, over a decade of experience.
10 : Face and brow presentation in northern Jordan, over a decade of experience.
11 : Obstetric malpresentations: twenty years' experience.
12 : Face and brow presentation: independent risk factors.
13 : Face presentation: predictors and delivery route.
14 : Management of fetal malpresentation.
15 : Racial differences in pelvic anatomy by magnetic resonance imaging.
16 : Assessment of race from the pelvis.
17 : Metric analysis of sex differences in South African black and white pelves.
18 : Shape variation in the human pelvis and limb skeleton: Implications for obstetric adaptation.
19 : The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations.
20 : Intrapartum translabial ultrasound demonstration of face presentation during first stage of labor.
21 : ISUOG Practice Guidelines: intrapartum ultrasound.
22 : Eyelid laceration in a neonate by fetal monitoring spiral electrode.
23 : Penetrating ocular injury with a fetal scalp monitoring spiral electrode.
24 : Neonatal eyelid penetration from insertion of a fetal scalp electrode: a case report.
25 : Face presentation at term.
26 : Face presentation.
27 : Face presentation in modern obstetrics--a study with special reference to fetal long term morbidity.
28 : Spinal cord injuries at birth: a multicenter review of nine cases.
29 : Spinal cord injuries at birth: a multicenter review of nine cases.
30 : Spinal cord injuries at birth: a multicenter review of nine cases.
31 : Spinal cord injuries at birth: a multicenter review of nine cases.
32 : Spinal cord injuries at birth: a multicenter review of nine cases.
33 : Persistent brow presentation: a new approach to management.
34 : Intrapartum bimanual tocolytic-assisted reversal of face presentation: preliminary report.
35 : Intrapartum bimanual tocolytic-assisted reversal of face presentation: preliminary report.
36 : Birth-related spinal cord injuries: a multicentric review of nine cases.
37 : Intrapartum translabial ultrasound demonstrating brow presentation during the second stage of labor.
38 : The effectiveness of intrapartum ultrasonography in assessing cervical dilatation, head station and position: A systematic review and meta-analysis.
39 : Brow presentation with vaginal delivery.
40 : Vaginal delivery of two cases of brow presentation using multiple Kiwi Omnicups.
آیا می خواهید مدیلیب را به صفحه اصلی خود اضافه کنید؟
اضافه کردن مدیلیب به صفحه اصلی

- Face Presentation

Pictoral Midwifery, Comyns Berkely, 4th Edition. 1941
Face it. We have a lot to learn about fetal positioning. The old paradigm is fetal positions are random. The new paradigm is that babies match the space available.
Face and brow presentations occur when baby’s spine extended until the head is shifted back so baby’s face comes through the pelvis first.
Baby may settle in a face or brow presentation before labor or they may become a face or brow presentation, usually when a posterior baby has it’s chin pushed further up by the pelvic floor during descent.
A baby who is in a face-first or forehead-first position often started as an extended (chin up) occiput posterior or occiput transverse position. Coming down on to the pelvic floor with the forehead leading then “converted” this baby’s head to the face first position.
The baby’s face may be bruised for a couple days after the birth. The brow presentation may cause a redness but only occasionally will cause a bruise.
Mobility of the pelvis and the freedom of maternal movements often help bring the face-first baby down through the pelvis with good strong, uterine surges.
But not always. Sometimes the labor can’t move baby down. Cesareans are more common, but a portion of the higher surgical rate is because time is not given to the mother to begin or continue labor, or to be out of bed for this labor. Monitoring becomes important. Expect a bit of an unusual heart rate to contraction pattern seen in these labors.
- When is Breech an Issue?
- Belly Mapping® Breech
- Flip a Breech
- When Baby Flips Head Down
- Breech & Bicornuate Uterus
- Breech for Providers
- What if My Breech Baby Doesn't Turn?
- Belly Mapping ®️ Method
- After Baby Turns
- Head Down is Not Enough
- Sideways/Transverse
- Asynclitism
- Oblique Lie
- Left Occiput Transverse
- Right Occiput Anterior
- Right Occiput Posterior
- Right Occiput Transverse
- Left Occiput Anterior
- OP Truths & Myths
- Anterior Placenta
- Body Balancing
What makes labor easier for a face-first baby and you?
Balance the body and the baby will thank you by curling into position to aim, not their face, but the crown of their head.
Flexion is physiological. So support physiology and the baby will change their position. We may need a little physics.
In Labor with a Face or Brow Presentation
Back baby up!
Forward-leaning Inversion with a jiggle of the buttocks right through 1-2 contractions often backs baby up so they can tuck their chin. Then they can aim into the pelvis with an easier position.

Shake the Apples in Forward-leaning Inversion with hands
A little effort can make labor a lot easier!
Only after baby’s crown is first, then do Side-lying Release in labor.
Before Labor with a face or brow presentation
Face presentation may reflect a psoas/pelvic floor imbalance with a collapse in the front body.
Free the piriformis, strengthen the buttocks, lengthen the hamstrings, squat for lengthening the pelvic floor, don’t worry about strengthening the pelvic floor right now. Alignment, walking, stabilizing and lengthening will tone the pelvic floor. Use it by breathing with your whole body.
Before labor, it’s safe to do Side-lying Release when baby’s face-first head isn’t in the pelvis yet.
Free the way
The psoas is the upper guide, the pelvic floor is the lower guide. release spasms and lengthen both.
Make room for the baby by releasing muscles that spasm, lengthen ligaments that are shortened, and support the abdominal muscles by attending to the muscles that interact with them, don’t go directly to the front first.

Contact to Listing Owner
Abnormal Fetal Position and Presentation
Under normal circumstances, a baby is in the vertex (cephalic) position before delivery. In the vertex position, the baby’s head is at the lower part of the abdomen, and the baby is born head-first. However, some babies present differently before delivery. In these cases, abnormal presentations may place the baby at risk of experiencing umbilical cord problems and/or a birth trauma (1). Types of abnormal fetal positions and presentations include the following. We’ll cover each in more detail on this page.
What is the difference between fetal presentation and position?
In the womb, a fetus has both a presentation and a position . Presentation refers to the baby’s body that leads, or is expected to lead, out of the birth canal (9). For example, if a baby’s rear is set to come out of the birth canal first, the baby is said to be in “breech presentation.” Position refers to the direction the baby is facing in relation to the mother’s spine (9). A baby could be lying face-first against a mother’s spine, or face up towards the mother’s belly.
What way should a baby come out during birth?
Vertex presentation is the ‘normal’ way that a baby is positioned for birth and the lowest-risk presentation for vaginal birth (1). In vertex presentation, the baby is positioned head-first with their occiput (the part of the head close to the base of the skull) entering the birth canal first. In this position, the baby’s chin is tucked into their chest and they are facing the mother’s back (occipito-anterior position). Any position other than vertex position is abnormal and can make vaginal delivery much more difficult or sometimes impossible (2). If a baby’s chin isn’t tucked into their chest, they may come out face-first (face presentation), which can cause birth injury (1).
What happens if a baby isn’t in the standard vertex position during birth?
Before delivery, it is critical that the fetus is in the standard vertex presentation and within the normal range for weight and size. This helps ensure the safety of both baby and mother during labor. When the baby’s size or position is abnormal, physician intervention is usually warranted (1). This may mean simple manual procedures to help reposition the baby or, in many cases, a planned C-section delivery . The failure of healthcare professionals to identify and quickly resolve issues related to fetal size, weight, and presentation is medical malpractice . There are numerous complications related to abnormal weight, size, abnormal position, or abnormal presentation.
Compound presentation
In the safest presentation (vertex presentation), the baby is born head first, with the rest of the body following. In a compound presentation, however, there are multiple presenting parts. Most commonly, this means that the baby’s head and an arm come out first at the same time. Sometimes compound presentation can occur with twins where the head of the first twin presents with the extremity of the second twin (3).
Risk factors for compound presentation include (3):
- Prematurity
- Intrauterine growth restriction (IUGR)
- Multiple gestations ( twins , triplets, etc.)
- Polyhydramnios
- A large pelvis
- External cephalic version
- Rupture of membranes at high station
Compound presentations can be detected via ultrasound before the mother’s water breaks. During labor, compound presentation is identified as an irregular finding during a cervical examination (3).
If a mother has polyhydramnios, the risk of compound presentation is higher, as the flow of amniotic fluid when the membranes rupture can sweep extremities into the birth canal, or cause a cord prolapse , which is a medical emergency (3). If compound presentation continues, it is likely to cause dystocia (the baby becoming stuck in the birth canal), which is also a medical emergency (3). Often, the safest way to deliver a baby with compound presentation is C-section, because complications like dystocia and cord prolapse carry risks of severe adverse outcomes, including cerebral palsy , intellectual and developmental disabilities, and hypoxic-ischemic encephalopathy (HIE) (3).
Limb presentation
Limb presentation during childbirth means that the part of the baby’s body that emerges first is a limb – an arm or a leg. Babies with limb presentation cannot be delivered safely via vaginal delivery; they must be delivered quickly by emergency C-section (4). Limb presentation poses a large risk for dystocia (the baby getting stuck on the mother’s pelvis), which is a medical emergency.
Occipitoposterior (OP) position
Approximately 1 out of 19 babies present in a posterior position rather than an anterior position. This is called an occipitoposterior (OP) position or occiput posterior position (3) In OP position, the baby is head-first with the back part of the head turned towards the mother’s back, rotated to the right (right occipitoposterior position, or ROP), or to the left (left occipitoposterior position, or LOP) of the sacroiliac joint. Occipitoposterior position increases the baby’s risk of experiencing prolonged labor , prolapsed umbilical cord , and use of delivery instruments, such as forceps and vacuum extractors (5). These conditions can cause brain bleeds , a lack of oxygen to the brain, and birth asphyxia .
When OP position is present, if a manual rotation cannot be quickly and effectively performed in the face of fetal distress, the baby should be delivered via C-section (5). A C-section can help prevent oxygen deprivation caused by prolonged labor, umbilical cord prolapse, or forceps and vacuum extractor use.
A nurse explains posterior position
Breech presentation
Breech presentation is normal throughout pregnancy. However, by the 37th week, the baby should turn to the cephalic position in time for labor. Breech presentation occurs when a baby’s buttocks or legs are positioned to descend the birth canal first. Breech positions are dangerous because when vaginal delivery is attempted, a baby is at increased risk for prolapsed umbilical cord, traumatic head injury, spinal cord fracture, fatality, and other serious problems with labor (6).
There are 4 types of breech positions:
- Footling breech presentation : In footling position, one or both feet enter the birth canal first, with the buttocks at a higher position than the feet.
- Kneeling breech presentation : This is when the baby has one or both legs extended at the hips and flexed at the knees.
- Frank breech presentation : This is when the baby’s buttocks present first, the legs are flexed at the hip and extended at the knees, and the feet are near the ears.
- Complete breech presentation : In this position, the baby’s hips and knees are flexed so that the baby is sitting cross-legged, with the feet beside the buttocks.
When a baby is in breech position, physicians often try to maneuver the baby into a head-first position. This should only be attempted if fetal heart tracings are normal (the baby is not in distress ) (7). The only type of breech position that may allow for a vaginal delivery is frank breech , and the following conditions must be met:
- The baby’s heart rate is being closely monitored and the baby is not in distress.
- Cephalopelvic disproportion (CPD) is not present; x-rays and ultrasound show that the size of the mother’s pelvis will allow a safe vaginal birth.
- The hospital is equipped for and the physician is skilled in performing an emergency C-section .
If these conditions are not present, vaginal birth should not be attempted. Most experts recommend C-section delivery for all types of breech positions because it is the safest method of delivery and it helps avoid birth injuries (6). Mismanaged breech birth can result in the following conditions:
- Brain bleeds, intracranial hemorrhages
- Spinal cord fractures
- Hypoxic-ischemic encephalopathy (HIE)
- Cerebral palsy
- Intellectual disabilities
- Developmental delays
Face presentation
A face presentation occurs when the face is the presenting part of the baby. In this position, the baby’s neck is deflexed (extended backward) so that the back of the head touches the baby’s back. This prevents head engagement and descent of the baby through the birth canal. In some cases of face presentation, the trauma of a vaginal delivery causes face deformation and fluid build-up (edema) in the face and upper airway, which often means the baby will need a breathing tube placed in the airway to maintain airway patency and assist breathing (1).
Image by healthhand.com
There are three types of face presentation:
- Mentum anterior (MA) : In this position, the chin is facing the front of the mother.
- Mentum posterior (MP) : The chin is facing the mother’s back, pointing down towards her buttocks in mentum posterior position. In this position, the baby’s head, neck, and shoulders enter the pelvis at the same time, and the pelvis is usually not large enough to accommodate this. Also, an open fetal mouth can push against the bone (sacrum) at the upper and back part of the pelvis, which also can prevent descent of the baby through the birth canal.
- Mentum transverse (MT) : The baby’s chin is facing the side of the birth canal in this position.
Trauma is very common during vaginal delivery of a baby in face presentation, so parents must be warned that their baby may be bruised and that a C-section is available to avoid this trauma.
Babies presenting face-first can sometimes be delivered vaginally, as long as the baby is in MA position (1). Safe vaginal delivery of a term-sized infant in persistent MP position is impossible due to the presenting part of the baby compared to the size of the mother’s pelvis (1). Babies in MP position must be delivered by C-section. Babies in MT position must also be delivered by C-section. Some babies in the MP and MT positions will spontaneously convert to the MA position during the course of labor, which makes vaginal delivery a possibility. If the baby is in the MA position and vaginal delivery is able to proceed, engagement of the presenting part of the baby probably will not occur until the face is at a +2 station (1).
The management of face presentation requires close observation of the progress of labor due to the high incidence of CPD with face presentation. In face presentation, the diameter of the presenting part of the head is, on average, 0.7 cm greater than in the normal vertex position (1).
In any face presentation situation, if progress in dilation and descent ceases despite adequate contractions, delivery must occur by C-section. In fact, when face presentation occurs, experts recommend liberal use of C-section (1).
Since there is an increased risk of trauma to the baby when the face presents, the physician should not try to rotate the baby internally. In addition, the physician must not use vacuum extractors or manual extraction (grasping the baby with hands) to extract the baby from the uterine cavity. Outlet forceps should only be used by experienced physicians; these forceps increase the risk of trauma and brain bleeds. In almost all clinical circumstances a cesarean delivery is the safest method of delivery.
Listed below are complications that can occur if face presentation is mismanaged by the medical team:
- Prolonged labor
- Facial trauma
- Facial and upper airway edema (fluid build-up in the face, often caused by trauma)
- Skull molding (abnormal head shape that results from pressure on the baby’s head during childbirth)
- Respiratory distress or difficulty in ventilation (the baby being able to move air in and out of lungs) due to upper airway trauma and edema
- Spinal cord injury
- Abnormal fetal heart rate patterns
- 10-fold increase in fetal compromise
- Brain bleeds
- Intracranial hemorrhages
- Permanent brain damage
Brow presentation
Brow presentation is similar to face presentation, but the baby’s neck is less extended. A fetus in brow presentation has the chin untucked, and the neck is extended slightly backward. As the term “brow presentation” suggests, the brow (forehead) is the part that is situated to go through the pelvis first. Vaginal delivery can be difficult or impossible with brow presentation, because the diameter of the presenting part of the head may be too big to safely fit through the pelvis.
Risk factors and conditions associated with brow presentation
Brow presentation has been linked to several risk factors and co-occurring conditions. These include:
- Multiparity (having previously given birth)
- Premature delivery
- Fetal anomalies such as anencephaly (an absence of major parts of the brain and skull) or anterior neck mass (a growth on the front of the neck)
- Previous c-section delivery
- Polyhydramnios (excessive amniotic fluid: infants swallow amniotic fluid while in utero, but this may be difficult if their neck is extended)
Diagnosis of brow presentation
Brow presentation can often be diagnosed through a vaginal examination during labor. If there are no conclusive signs from the physical examination alone, an ultrasound can also be used. Warning signs of brow presentation may include signs of fetal distress or lack of labor progression.
Management of brow presentation
Infants who assume a brow presentation early in labor may spontaneously move into a more optimal position during the delivery process. Additionally, safe delivery in brow presentation may be possible if the infant is unusually small and/or the mother’s pelvic opening is unusually large. For these reasons, physicians occasionally recommend vaginal delivery of infants in brow presentation.
Doctors attempting vaginal delivery of a baby in brow presentation must be very careful to watch for signs of fetal distress (such as an abnormal heart rate), and to monitor the progression of labor. Prolonged labor can cause extended periods of fetal oxygen deprivation, which can cause birth asphyxia and permanent injury. Signs of fetal distress can indicate that a baby is in danger of sustaining serious brain damage if action is not quickly taken to prevent this. If an infant in brow presentation begins to show signs of distress, or if labor progress stops or slows significantly, physicians should be ready to move on to a cesarean delivery.
Labor induction or augmentation with the drug Pitocin (synthetic oxytocin) is very dangerous in cases of brow presentation. Pitocin can lead to excessive uterine contractions, which can put pressure on the infant’s head and cut off their oxygen supply; this is especially risky when safe fetal descent is already compromised, such as in cases of brow presentation.
Complications of brow presentation
If brow presentation is diagnosed in a timely fashion and is appropriately managed, there are typically no serious negative effects on the mother or baby. However, if medical professionals fail to recognize brow presentation and intervene as necessary, there can be lasting consequences. Infants may suffer oxygen deprivation due to prolonged labor, or traumatic injuries from a difficult delivery. Some of the most severe conditions resulting from mismanaged brow presentation births include:
- Hypoxic-ischemic encephalopathy
- Periventricular leukomalacia
- Seizure disorders
- Developmental disabilities
Shoulder presentation (transverse lie)
Shoulder presentation (transverse lie) is when the arm, shoulder or trunk of the baby enter the birth canal first. When a baby is in a transverse lie position during labor, C-section is almost always used as the delivery method (8). Mothers who have polyhydramnios (too much amniotic fluid), are pregnant with more than one baby, have placenta previa, or have a baby with intrauterine growth restriction (IUGR) are more likely to have a baby in the transverse lie position (8). Once the membranes rupture, there is an increased risk of umbilical cord prolapse in this position; thus, a C-section should ideally be performed before the membranes break (8). Failure to quickly deliver the baby by C-section when transverse lie presentation is present can cause severe birth asphyxia due to cord compression and trauma to the baby. This can cause hypoxic-ischemic encephalopathy (HIE), seizures, permanent brain damage, and cerebral palsy.
Legal help for birth injuries from abnormal position or presentation
The award-winning birth injury attorneys at ABC Law Centers: Birth Injury Lawyers have over 100 years of joint experience handling birth trauma cases related to abnormal position or presentation. If you believe your loved one’s birth injury resulted from an instance of medical malpractice, you may be entitled to compensation from a medical malpractice or personal injury case. During your free legal consultation, our birth injury attorneys will discuss your case with you, determine if negligence caused your loved one’s injuries, identify the negligent party, and discuss your legal options with you.
- Free Case Review
- Available 24/7
- No Fee Unless We Win
Featured Videos
Testimonial from keziah’s family, posterior position, hypoxic-ischemic encephalopathy (hie).
Featured Testimonial
What Our Clients Say…
After the traumatic birth of my son, I was left confused, afraid, and seeking answers. We needed someone we could trust and depend on . ABC Law Centers: Birth Injury Lawyers was just that.
Helpful resources
More about our firm.
- Meet our birth injury attorneys
- Meet our in-house medical staff
- Verdicts and settlements
- Testimonials
- Julien, S., and Galerneau, F. (2017). Face and brow presentations in labor. Retrieved from https://www.uptodate.com/contents/face-and-brow-presentations-in-labor .
- World Health Organization, UNICEF, and United Nations Population Fund. Malpositions and malpresentations. Retrieved from http://hetv.org/resources/reproductive-health/impac/Symptoms/Malpositions__malpresetations_S69_S81.html .
- Barth, W. (2016). Compound fetal presentation. Retrieved from https://www.uptodate.com/contents/compound-fetal-presentation .
- Gabbe, S.G., … Grobman, W.A. (2017). Compound Presentation. Retrieved from https://expertconsult.inkling.com/read/gabbe-obstetrics-normal-problem-pregnancies-7e/chapter-17/compound-presentation .
- Argani, C.H. and Satin, A.J. (2018) Occiput posterior position. Retrieved from https://www.uptodate.com/contents/occiput-posterior-position .
- Hofmeyr, G.J. (2018). Overview of issues related to breech presentation. Retrieved from https://www.uptodate.com/contents/overview-of-issues-related-to-breech-presentation .
- Hofmeyr, G.J. (2017). Delivery of the fetus in breech presentation. Retrieved from https://www.uptodate.com/contents/delivery-of-the-fetus-in-breech-presentation .
- Strauss, R.A. (2017). Transverse fetal lie. Retrieved from https://www.uptodate.com/contents/transverse-fetal-lie .
- Moldenhauer, J.S. (2018). Abnormal Position and Presentation of the Fetus. Retrieved from https://www.merckmanuals.com/home/women-s-health-issues/complications-of-labor-and-delivery/abnormal-position-and-presentation-of-the-fetus .
Over $350 Million Recovered
In Verdicts, Settlements, & Judgements
$4.75 Million
$3.9 Million
$5.85 Million
Awards & Memberships
- Vishal's account
- Complications
Brow Presentation – An Overview

What Is Brow Presentation?
How can you get to know if your baby is in this position, what are the causes of brow presentation, how is the diagnosis made, complications of brow presentation delivery, alternatives for labor during brow presentation, precautions to take before and after labour, how will brow presentation affect your baby during labor.
Pregnancy is a beautiful experience that is also fraught with a host of complications and risks. One of them concerns the normal orientation of your baby inside your uterus, which is essential for a smooth delivery. This article will explain all about abnormal forehead presentation and its associated causes, complications, diagnosis, treatment and precautions.
Babies assume a fixed position in the uterus, that is with their chins tucked firmly into their chests. This position is ideal to exit the uterus smoothly. However, in some cases, the baby’s head and neck will extend backwards away from their chest. This is known as a brow presentation or forehead presentation. It is an extremely rare condition, occurring once in 1500 births. Brow presentation might obstruct vaginal births from occurring as there is less space for the baby to drop down towards the pelvic girdle. However, if brow presentation occurs early in labour, there is still time for them to flex their neck back to the right position. If not, labour might be hindered, causing stress for both, the mother and the baby. In these instances, your doctor might recommend a caesarean section. A brow baby tends to occur in women pregnant for the second or third time, or due to physical defects like an abnormally developed spine.
Brow babies are rarely detected before labor begins, but around half of them will shift to a face-first or crown-first presentation suitable for delivery. A brow presentation delivery will take much longer than normal, which is usually when the condition is discovered.
There are several potential reasons for your baby to assume this orientation. Some of them are:
- Fetal Size: Babies born preterm, or with low birth weights, raise the likelihood of them presenting brow first. This is also observed in large babies, who usually flex their head outwards rather than in towards their chest. Brow presentation can also be caused if your pelvic girdle and your baby’s head are disproportionate to each other.
- Polyhydramnios: Polyhydramnios is the condition in which there is too much amniotic fluid in your uterus. Thus, it might be tricky for your baby to fix their heads in the correct position.
- Multiple Pregnancy: Carrying twins or more in your womb decreases the amount of space available, making your babies take alternative positions to fit properly.
- Maternal Defects: If your pelvis is not the right shape and size, it might be difficult for your fetus to assume normal presentations. The most common cause of brow presentation is the triangle-shaped android pelvis and the atypically small contracted pelvis. Another maternal defect is a lax uterus, which is not firm enough to hold the baby in place, resulting in different presentations.
- Fetal Defects: If your baby has conditions such as anencephaly and hydrocephalus, their abnormally large heads will not be able to take the right position.
To diagnose brow presentation, an experienced doctor will be able to help. Ultrasound scans are compulsory for monitoring the situation. Your doctor might even conduct a digital examination to check the orientation of the baby’s facial features. If they find that the baby’s head does not rotate enough for a natural birth, they might recommend a caesarean section.
Several risks come with brow presentation birth. Some of them are:
- Labor time might be extended as the baby would have a hard time getting past the pelvis.
- Forceps might be required, which could cause cranial damage.
- Baby’s head shape might be altered due to difficulty while moving through the birth canal.
- Baby may go through stress during delivery as it would be difficult birth and may require a caesarean.
- Injuries may occur to the baby’s spinal cord due to trauma.
- Increased risk of cerebral hemorrhage in the baby as the head may take in damage.
As explained already, a baby in brow presentation might not have enough space to move downwards towards the cervix. If this happens, there are a few methods your doctor might implement to reduce the complications of natural birth. These methods require medical skill and enough space within the cervix to be attempted.
- Ventouse Birth: In this case, your doctor will use a small vacuum extraction device known as a ventouse to pull the baby’s head towards their chest. This method can be used even after you have begun to push.
- Manual Rotation: After the cervix undergoes complete dilation, your doctor might attempt to move the baby’s head into the correct position using their hands.
As there are several complications linked with brow presentations, here are some precautions for you to take before and after labour to have a successful pregnancy.
- Choose a doctor who is accomplished in obstetrics and gynaecology, so they are experienced in dealing with any potential outcome.
- Visit your doctor regularly, especially at the end of your third trimester.
- If you have been diagnosed with brow presentation, do not hesitate to go for a caesarean if strongly recommended by your doctor, as it dramatically reduces the risks involved.
Babies might end up with abnormally shaped heads if they go through vaginal birth with a brow presentation. However, as their heads are malleable, they will return to a normal shape in a few days. Extended labor might cause stress in your baby who has been stuck in an uncomfortable position the whole time. This might also lead to vertebral problems, so consult a paediatric osteopath if you are concerned.
Brow presentation can happen to anyone, so not encountering it in your first pregnancy does not mean you will not see during later pregnancies. Consume a balanced, nutritious diet, stay hydrated and get enough sleep. Avoiding tension and anxiety will help you stay strong for when your baby arrives.
Also Read : Preparing for Labour & Delivery – Smart Ways to Prepare for Childbirth

- RELATED ARTICLES
- MORE FROM AUTHOR

Medical Abortion - Procedures, Risks and Side Effects

Subchorionic Hemorrhage - Causes & Treatment

Placenta During Pregnancy - Functions & Complications

Meet The Real Life Miracle Baby Born to a Mom With No Muscles!

Uterine Rupture - Causes, Symptoms and Treatment
")
Intrauterine Growth Restriction (IUGR)
Popular on parenting.

245 Rare Boy & Girl Names with Meanings

Top 22 Short Moral Stories For Kids

170 Boy & Girl Names That Mean 'Gift from God'

800+ Unique & Cute Nicknames for Boys & Girls
Latest posts.

Father's Day Coloring Pages - Free Printables For Kids
Happy father's day animated gifs worth sharing.

Spiderman Coloring Pages - Free Printable Pages For Kids

Hamster Coloring Pages - Free Printable Pages For Kids
- Share full article
Advertisement
Supported by
Guest Essay
Something’s Rotten About the Justices Taking So Long on Trump’s Immunity Case

By Leah Litman
Ms. Litman is a professor at the University of Michigan Law School, a host of the “Strict Scrutiny” podcast and a former clerk to the Supreme Court justice Anthony Kennedy.
For those looking for the hidden hand of politics in what the Supreme Court does, there’s plenty of reason for suspicion on Donald Trump’s as-yet-undecided immunity case given its urgency. There are, of course, explanations that have nothing to do with politics for why a ruling still hasn’t been issued. But the reasons to think something is rotten at the court are impossible to ignore.
On Feb. 28, the justices agreed to hear Mr. Trump’s claim that he is immune from prosecution on charges that he plotted to subvert the 2020 election. The court scheduled oral arguments in the case for the end of April. That eight-week interval is much quicker than the ordinary Supreme Court briefing process, which usually extends for at least 10 weeks . But it’s considerably more drawn out than the schedule the court established earlier this year on a challenge from Colorado after that state took Mr. Trump off its presidential primary ballot. The court agreed to hear arguments on the case a mere month after accepting it and issued its decision less than a month after the argument. Mr. Trump prevailed, 9-0.
Nearly two months have passed since the justices heard lawyers for the former president and for the special counsel’s office argue the immunity case. The court is dominated by conservatives nominated by Republican presidents. Every passing day further delays a potential trial on charges related to Mr. Trump’s efforts to remain in office after losing the 2020 election and his role in the events that led to the storming of the Capitol; indeed, at this point, even if the court rules that Mr. Trump has limited or no immunity, it is unlikely a verdict will be delivered before the election.
The immunity case is not the only big case hanging fire. Some two dozen remain undecided that were argued even before the April 25 oral argument over Mr. Trump’s immunity. A case on gun rights for domestic abusers under a restraining order was argued in November; cases involving the power of federal agencies and a multibillion-dollar settlement for opioid victims were heard in December and January; the court also has yet to decide whether upwind states must cut emissions that affect the air quality in downwind states. That case was argued in February.
The court is a busy place, though the justices are completing decisions at the second slowest rate since the 1946 term, according to a recent article in The Wall Street Journal. The court tries to wrap up its business for the term that began in October by the end of June. It’s not shocking that cases argued later in the term end up being decided later, especially because by the end of April, when the immunity case was heard, the court was still working to finish cases argued months earlier. April was also among the court’s busiest months: The justices heard 10 cases.
But these seemingly mundane, process explanations overlook some of the particulars in the immunity case. Mr. Trump’s lawyers put together a set of arguments that are so outlandish they shouldn’t take much time to dispatch. Among them is the upside-down claim that, because the Constitution specifies that an officer who is convicted in an impeachment proceeding may subsequently face a criminal trial, the Constitution actually requires an impeachment conviction before there is any criminal punishment.
We are having trouble retrieving the article content.
Please enable JavaScript in your browser settings.
Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.
Thank you for your patience while we verify access.
Already a subscriber? Log in .
Want all of The Times? Subscribe .
Lesson Plan
June 17, 2024, 6:05 a.m.
Lesson plan: History of Juneteenth and why it became a national holiday

A Juneteenth celebration in Richmond, Virginia, 1905. Library of Congress
This lesson was originally published on June 16, 2021, and was updated on June 16, 2024.
For a Google version of this lesson plan, click here . (Note: you will need to make a copy of the document to edit it).
In this lesson, students will explore and discuss the history and context around the Juneteenth holiday in the United States. Topics explored will include the history of racial injustice in the U.S., the Civil War and the limitations of the Emancipation Proclamation. Additionally, students will be encouraged to explore the modern significance of Juneteenth and its long-term impact.
Estimated time
One 50-60 minute class period
Grade Level
Grades 6-12
On June 15, 2021, the Senate unanimously approved a bill approving June 19 as a federal holiday for “Juneteenth National Independence Day.” The House passed the bill one day later. Still, many Americans are still unaware of the history and significance of June 19.
On Jan. 1, 1863, President Abraham Lincoln issued the Emancipation Proclamation declaring “that all persons held as slaves” in the Confederacy “shall be free.” While this may have freed some enslaved people on paper, the reality was much more complicated.

Source: PBS NewsHour via Associated Press
For instance, the Emancipation Proclamation only freed those slaves held under the Confederacy, not in border states loyal to the Union, including Kentucky, West Virginia and Delaware, where slavery was still legal after the Emancipation Proclamation. In fact, slavery was still legal in Kentucky until Dec. 1865, when the 13th Amendment was passed, though Kentucky voted against ratifying the amendment.
Confederate states and slaveholders also resisted emancipation, and many people remained enslaved in Confederate states after the proclamation, even as many enslaved people fought for their freedom or escaped behind Union lines. On June 19, 1865, Major General Gordon Granger of the Union issued an order in Galveston, Texas, alerting all enslaved persons that they were legally free.
At this point in 1865, Texas was the westernmost state in America and one of the last Confederate states to be occupied by the Union. Many slaveholders had fled Union advances in other parts of the South to Texas, along with the people they had enslaved.
While it took time for the logistics of “freeing” enslaved people to come into effect, the importance of June 19, or “Juneteenth” lived on. Considering how complicated emancipation was, many dates were considered for holding celebrations of emancipation, but over 150 years later, June 19 remains.
What originally was a holiday mainly observed by Texans has grown to be recognized all over the country. Each year on “Juneteenth,” (or more formally Juneteenth National Freedom Day), communities all around the United States gather and celebrate and reflect on the history of slavery and struggle for civil rights and equality, including the work that still remains after conditional advances such as the Emancipation Proclamation.
Warm up activity
As a class, watch the BrainPop video (8 minutes) below found here introducing Juneteenth. While watching the video, answer the following discussion questions.

Source: BrainPop
Discussion questions:
- What is “Juneteenth”? What does it celebrate?
- Why did it take so long for enslaved peoples in Texas to finally be free? What obstacles existed?
- What were some of the forms of discrimination against newly freed people mentioned in the video?
- What is the Great Migration?
- How did Juneteenth become a national, not just regional, celebration?
After watching the video, separate into groups of 3-4 to discuss the focus questions (5 minutes).
Main activities:
- Why was June 19th chosen as the date to celebrate the freedom of all Americans? What were some of the drawbacks to other dates? Can you make an argument for why you think a different date might have been better and/or worse?
- Gates describes several reasons why Juneteenth struggled to be remembered at times, and why it was able to endure. Compare and contrast what the BrainPop video included as reasons why Juneteenth struggled and endured with what Gate’s emphasizes. What do you think were the most important factors in Juneteenth’s momentum and remembrance continuing?
- “When did they start recognizing Juneteenth, if at all?”
- “What was the process of Juneteenth becoming a holiday in my state?”
- If Juneteenth isn’t recognized in your state, see if you can answer, “Why is Juneteenth not recognized?”
- This search engine for state and local government websites
- The Library of Congress
Additional activities
- Brainstorm or plan a Juneteenth celebration activity. This can be decorating a common area, bringing in a relevant local speaker or planning a refreshment break for your school. Juneteenth celebrations can be in the home, at school or in community locations. For more inspiration see these resources:
- “ How to Celebrate ” from Juneteenth.com
- See how others are celebrating Juneteenth on Twitter .
- Some activists feel ambivalent about Juneteenth becoming a national holiday, or reject the idea. To learn more about the nuances surrounding making Juneteenth a federal holiday, watch this NewsHour interview with Dr. Mark Anthony Neal recorded in 2020 amid the George Floyd protests.
- The day now known as Juneteenth was formally recognized as a national holiday in 2021, due in large part to the activism of retired teacher Opal Lee. Learn more about Lee's activism and the message of Juneteenth in this NewsHour interview with Opal Lee.
If classrooms finish and plan a celebratory activity, please share your ideas with us on social media @NewsHourEXTRA on Twitter.
This lesson was written by Cecilia Curran, NewsHour Classroom intern, while she was a rising sophomore at Amherst College. This lesson was edited by NewsHour Classroom's education producer and former history teacher Vic Pasquantonio.
Fill out this form to share your thoughts on Classroom’s resources. Sign up for NewsHour Classroom’s ready-to-go Daily News Lessons delivered to your inbox each morning.
Recent Lesson Plans

Lesson Plan: Political Parties: Two is Company, Three’s a Crowd
The Founders did not intend to create a two-party system and yet that is exactly what has thrived in American history. But what about the role of third-party candidates?

Lesson Plan: Using robotics to support rural communities
A short project-based lesson that weaves arts & sciences together

Lesson plan: Watergate and the limits of presidential power
On August 9, 1974, President Richard M. Nixon resigned from the Oval Office. Use this resource to teach young people about this period in U.S. history.

How2Internet: Use media literacy skills to navigate the misinformation highway
Learn to produce a fact-check video using media literacy skills
- government-civics
- social-studies
- social-issues
- news-media-literacy
- lesson plan
SUPPORTED BY VIEWERS LIKE YOU. ADDITIONAL SUPPORT PROVIDED BY:
Copyright © 2023 NewsHour Production LLC. All Rights Reserved
Illustrations by Annamaria Ward
- Case report
- Open access
- Published: 15 June 2024
An incidental finding of a hemoglobin E variant in a diabetic patient with an abnormal glycated hemoglobin level: a case report
- Rashmi Karki 1 na1 ,
- Samir Lamichhane ORCID: orcid.org/0000-0003-0748-0767 2 na1 ,
- Runa Jha 1 &
- Rekha Manandhar 1 na1
Journal of Medical Case Reports volume 18 , Article number: 279 ( 2024 ) Cite this article
479 Accesses
1 Altmetric
Metrics details
Glycated hemoglobin is a well-known marker for evaluating long-term glycemic control. However, the accuracy of glycated hemoglobin measurement can be affected by the presence of hemoglobin variants, which makes the determination and interpretation of glycated hemoglobin values in terms of glycemic control not only difficult but also misleading. Here we present the first ever case of a patient with type 2 diabetes with hemoglobin E from Nepal, diagnosed incidentally because of spurious glycated hemoglobin levels.
Case presentation
A 45-year-old Hindu Mongolian female with a history of type 2 diabetes for around 9 years but not very compliant with follow-ups was referred to our facility for plasma fasting and postprandial blood glucose levels and glycated hemoglobin. Fasting and postprandial blood sugars were found to be high. A consistent very low glycated hemoglobin by two different high-performance liquid chromatography (HPLC) methods compelled us to call the patient for a detailed clinical history and for the records of investigations done in the past. The patient has been a known case of type 2 diabetes for around 9 years and presented irregularly for follow-up visits. Around 4 years ago, she presented to a healthcare facility with fatigue, severe headaches, pain in the abdomen, discomfort, and dizziness for a couple of months, where she was shown to have high blood glucose. She was referred to a tertiary-level hospital in Kathmandu, where she was prescribed metformin 500 mg once daily (OD). Due to her abnormal hemoglobin A1c reports, she was then sent to the National Public Health Laboratory for repeat investigations. Her blood and urine investigations were sent. Complete blood count findings revealed high red blood cell and white blood cell counts, a low mean corpuscular volume, and a high red cell distribution width-coefficient of variation. Other parameters, including serum electrolytes, renal function tests, liver function tests, and urine routine examinations, were within normal limits. A peripheral blood smear revealed microcytic hypochromic red cells with some target cells. Hemoglobin electrophoresis showed a very high percentage of hemoglobin E, a very low percentage of hemoglobin A2, and normal proportions of hemoglobin A and hemoglobin F. A diagnosis of homozygous hemoglobin E was made, and family screening was advised.
Conclusions
Clinicians should be aware of the limitations of glycated hemoglobin estimation by ion exchange high-performance liquid chromatography in patients with hemoglobin E and other hemoglobin variants. If the clinical impression and glycated hemoglobin test results do not match, glycated hemoglobin values should be determined with a second method based on a different principle, and glycemic status should be confirmed through alternative investigations, preferably those that are not influenced by the presence of hemoglobin variants (for example, boronate affinity chromatography, fructosamine test, glycated albumin test, the oral glucose tolerance test, continuous glucose monitoring, etc.). Consistent or even doubtful results should also raise the suspicion of a hemoglobin variant, which should be confirmed through further evaluation and investigations.
Peer Review reports
Introduction
Glycated hemoglobin (HbA1c), initially identified as “unusual” hemoglobin in patients with diabetes over half a century ago [ 1 ], has now become a well-known marker of long-term glycemic control in individuals with diabetes mellitus [ 2 ], reflecting an average blood glucose level over a period of around 3 months. Glycemic control being an important factor for the progression to long-term complications, HbA1c strongly correlates with the risk of developing chronic complications associated with diabetes as well [ 3 ]; hence, it has become not only a diagnostic tool but also a screening tool for individuals at risk of diabetes [ 4 ]. However, the accuracy of HbA1c measurement can be affected by various factors such as erythropoiesis, glycation, erythrocyte destruction, and the presence of hemoglobin (Hb) variants [ 5 ], which makes the determination and interpretation of HbA1c values in terms of glycemic control not only difficult but also misleading [ 6 ]. Here, we present a case of a variant of Hb, the HbE, diagnosed incidentally in a patient with type 2 diabetes mellitus suspected initially because of repeated abnormal HbA1c levels detected with an ion-exchange high-performance liquid chromatography (HPLC) and hence subjected to further investigations by Hb capillary electrophoresis to confirm the diagnosis. To our knowledge, this is the first ever incidentally diagnosed case of HbE in a patient with type 2 diabetes from Nepal, all because of spurious HbA1c levels.
A 45-year-old Hindu Mongolian female, with a history of type 2 diabetes for 9 years and under medication for the last 4 months, visited the National Public Health Laboratory (NPHL), Teku, to test for plasma fasting and postprandial blood glucose levels and HbA1c.
We tested HbA1c by high-performance liquid chromatography (HPLC) Biorad VARIANT II, which showed HbA1c to be only 1.1% (Fig. 1 ). The control test run for the day was within range. Fasting and postprandial blood sugars were found to be 173 mg/dL and 280 mg/dL, respectively. The patient sample was rechecked with HPLC TOSO 7234X, which showed HbA1c of 2.1%. In view of this, the patient was contacted and advised to have a complete blood count (CBC) and hemoglobin electrophoresis. We took a detailed history of the patient and requested the records of investigations done in the past.

HbA1c detection by HPLC
According to the patient, she was apparently well around 9 years ago (the patient herself was not sure about the exact date) when she started developing increased urination, increased thirst, weakness, and occasional dizziness for a couple of months. She then visited a local health care facility near her hometown, where she was examined and sent for some blood and urine investigations (she has misplaced the lab reports, or probably lost them, according to her). According to her, she was told that she has high blood sugar levels and was advised to make some lifestyle modifications, such as dietary changes and increasing physical activities. She was also prescribed medication (she has no records of the medications prescribed then) and was asked to follow up in the next 3 months. Thereafter, she was doing fine with no complaints for a couple of years, and she never followed up with any healthcare facility until around 3–4 years ago (May 2020), when she presented herself to a healthcare facility in Kathmandu city with complaints of fatigue, severe headaches, pain and discomfort in the abdomen, and occasional dizziness and a feeling of lightheadedness for a couple of months. She also complained of weakness and decreased tolerance for physical activity. Physical examination was unremarkable, and laboratory investigations revealed high blood glucose and serum triglyceride levels (fasting blood glucose: 175 mg/dL; postprandial blood glucose: 193 mg/dL; serum triglyceride: 290 mg/dL). Other investigations were within normal limits (Table 1 ).
With these reports, she was referred to a tertiary-level hospital in Kathmandu. On 1 January 2021, she visited Shree Birendra Hospital (a tertiary-level hospital in Kathmandu), where she was further evaluated. At this time, she also admitted having a history of a slight decrease in vision for the last few months and was evaluated for any eye findings. Apart from a slightly presbyopic finding, everything else was normal. Intraocular pressure was within normal limits. There were no findings suggestive of diabetic retinopathy. The fundus examination was normal. Further lab workup findings revealed the following: TLC: 11,660 cells/mcL; Differential Count (DC): Neutrophils = 76, Lymphocytes = 17, Monocytes = 5, Eosinophils = 1, Basophils = 1; MCV: 64.4 fL; MCH: 21.9 pg; RDW-SD: 36.1 fL; RDW-CV: 17.3 fL; postprandial (PP) blood glucose (two hours after taking a meal): 294 mg/dL; and HbA1c: 2.1%. Ultrasonography (USG) of the abdomen and pelvis showed a bulky uterus. All other investigations were within normal limits (Table 1 ).
She was prescribed metformin 500 mg OD and advised to make lifestyle modifications once again. She was then referred to the National Public Health Laboratory (NPHL), the central reference laboratory in Nepal, for repeat investigations to confirm the abnormal HbA1c reports and for all other relevant investigations. On arrival at NPHL (21 January 2021), she was thoroughly interviewed for a detailed medical history. She was a nonvegetarian, and she did not smoke tobacco or consume alcohol. She had never received a blood transfusion before. Apart from the metformin prescribed earlier, she was not on any other medications. There was no family history of low hemoglobin levels or blood transfusions. There was no other significant medical history in any of her family members, as far as the patient could remember. She gave a history of iron supplementation a long time ago (around 9 years ago when she first presented to a healthcare facility) for around 3 months but not thereafter. She denies any history of any means of blood loss. She has been married for around 25 years and has two kids (elder son: 23 years old, younger daughter: 21 years old). Physical examination was unremarkable and provided the following data: height: 5 feet; weight: 68 kg; body mass index (BMI): 29.3. Laboratory investigations are as follows:
CBC findings revealed hemoglobin of 13.6 g/dL, RBC of 6.2 × 10 6 cells/mcL, total leucocyte counts of 13,700 cells/mcL ( N = 77, L = 18, M = 4, E = 1, B = 0), platelet count of 2.8 × 10 5 cells/mcL, and packed cell volume (PCV) of 42.1%. Red cell indices included mean corpuscular volume (MCV), mean hemoglobin concentration (MCH), mean corpuscular hemoglobin concentration (MCHC), and RDW-CV%, which were found to be 67 fL, 21.7 pg, 32.3 g/dL, and 17.9%, respectively. All other investigations were within normal limits (Table 1 ).
The ultrasonography (USG) report of the abdomen and pelvis revealed a bulky uterus and was otherwise unremarkable.
Hb electrophoresis was performed in the SEBIA MINICAP FLEX PIERCING electrophoretogram, which showed 93.2% HbE, 2.4% HbA2, 2.9% HbF, and 1.5% HbA (Fig. 2 ). A peripheral blood smear revealed microcytic hypochromic red cells with some target cells. White blood cell (WBC) and platelet morphology seem to have no abnormalities.

Detection of HbE by capillary electrophoresis
On the basis od these findings, a diagnosis of homozygous HbE was made, and family screening was advised.
Discussion and conclusion
Glycated hemoglobin (HbA1c), an effective and objective retrospective marker reflecting an average blood glucose level over a period of around 3 months, has now become a well-known indicator of long-term glycemic control in individuals with diabetes mellitus. However, there are various factors that may influence and falsely alter the level of HbA1c and its measurement and hence need to be considered in patients with abnormal readings.
HbA1c levels seem to inversely correlate with the rate of erythropoiesis, and hence factors that decrease the rate of erythropoiesis (including iron, vitamin B 12 , and folate deficiency) and/or increase erythrocyte life span (for example, due to splenectomy) falsely increase the level of HbA1c. Conversely, administration of erythropoietin, iron, and vitamin B 12 and conditions associated with reticulocytosis and decreased erythrocyte lifespan (for example, splenomegaly or even pregnancy) tend to falsely decrease the level of HbA1c [ 1 , 7 ]. There has been evidence of a false increase in HbA1c in cases of alcoholism and in patients with chronic kidney disease (CKD), as well, possibly through the same mechanism (alcohol interferes with folate metabolism, and patients with CKD have decreased erythropoietin levels) [ 1 , 7 , 8 ]. Several other conditions, for example, hyperbilirubinemia, carbamylated hemoglobin, chronic opiate use, etc., are also seen to be associated with a high HbA1c level [ 1 ]. However, chronic liver disease, rheumatoid arthritis, hypertriglyceridemia, and even the use of drugs such as ribavirin and dapsone have been shown to be associated with decreased HbA1c [ 1 , 7 , 9 , 10 ]. Genetic or chemical alterations in hemoglobin undoubtedly have some associations with HbA1c, and hence certain hemoglobinopathies, including the HbE disease, the presence of HbF, and methemoglobinemia, may also alter the level of HbA1c [ 1 , 7 , 11 ]. Here we discuss the presence of HbE and the misleading value of HbA1c levels.
Hemoglobin E, a variant hemoglobin, is characterized by a mutation in the β globin gene ( HBB gene) causing substitution of glutamic acid for lysine at position 26 of the β globin chain, resulting in a heterogeneous group of disorders whose phenotypes range from asymptomatic to severe disease [ 12 , 13 ]. HbE trait and HbEE are mild disorders, while a combination of HbE with other forms of hemoglobinopathies does exist that can have a markedly different and more serious clinical course, producing a wide range of clinical syndromes of varying severity [ 13 , 14 ]. The heterozygous form of HbE is usually characterized by minimal red cell morphological abnormalities and normal red cell indices, while homozygotes for HbE can have red cells with significant morphological abnormalities, including increased numbers of target cells, and can present with mild microcytic hypochromic anemia [ 14 ].
Despite advances in the standardization of methods for glycohemoglobins, including HbA1c, an increasing number of hemoglobinopathies have been shown to interfere with the accurate measurements and determination of these glycohemoglobins. Even the most commonly used methods, that is, the HPLC methods for HbA1c determination, lacked the resolution necessary to differentiate hemoglobin variants [ 6 ]. The demonstration of additional peaks in the chromatograms and either too low or too high values of HbA1c has been shown as compared with the nondiabetic reference range in different types of hemoglobinopathies [ 15 ].
Patients homozygous for HbE, that is, those receiving mutated genes from both parents, have a very low HbA level, with around 80% of Hb being HbE itself. The mutation associated with HbE tends to alter the ionic charges on Hb and hence interferes with the measurement of HbA1c via the ion-exchange HPLC method, especially in homozygous cases [ 16 , 17 ]. Unique mutation(s) on the N-terminal of β-globin in some hemoglobinopathies such as the Hb Graz and the Hb Long Island variants also seem to cause inappropriately high and low apparent HbA1c titers via HPLC methods. However, estimations with the boronate affinity technique and the immunoassay technique seem to be unaffected. The boronate affinity method has shown values in an acceptable and clinically reasonable range for all hemoglobin variants, as evidenced by several studies [ 18 , 19 ]. In fact, affinity methods have already been suggested as an acceptable and more useful method for reflecting glycemic control because they mainly measure glycohemoglobin regardless of the glycation site and hence may be clinically more accurate [ 15 ]. Studies have shown that results from the HbA1c immunoassays were also comparable to those from HPLC assays, showing good correlation, appropriate precision, and low bias [ 20 ]. Immunoassays utilizing various antibodies raised against specific epitopes of hemoglobin, for example, the Amadori product of glucose plus the first eight amino acids on the N-terminal end of the beta chain of hemoglobin, and many more, have shown good correlation with established methods for estimating glycohemoglobin [ 21 ]. However, as the quality of an immunoassay typically depends on the specificity of the antibody to the specific epitope on HbA, specific mutations altering the common epitopes used for the assays will hinder the accuracy of the test. One such example includes the hemoglobin variant with mutations affecting or altering the epitope at the N-terminal chain. The mutation seems to affect the ability of the monoclonal antibody that is used in the assay to detect hemoglobin [ 22 ]. Some uncommonly occurring variants that span the commonly used epitope include HbE and HbD (Los Angeles), where mutations occur at β26 and β121, respectively. There are some other evidences/studies that have reported that immunoassays have been shown to produce false HbA1c results in certain Hb variants [ 23 , 24 , 25 , 26 ]. Hence, choosing a method where the antibody epitope does not span the specific area in the Hb variant is crucial. However, it is not practical or even feasible to produce several specific antibodies (according to the individual patient) at each facility, and hence understanding the effects of such hemoglobinopathies while estimating the glycohemoglobins is crucial. To be precise, the effect of various hemoglobinopathies on HbA1c measurements is highly method-dependent. So, it is always better to be correlated clinically, and whenever the HbA1c results do not fit the clinical picture, some additional peaks in HPLC chromatograms are displayed, or any such doubtful scenario has been presented, it should not be ignored, and further investigations are advisable. Glycemic status over a short period of time (1–3 weeks) can also be reflected by the fructosamine test. Some researchers have therefore recommended confirmation with the fructosamine test or the glycated albumin test as an alternative [ 14 , 24 , 27 , 28 ]. Fructosamine results depend on the glycation of serum proteins and are not influenced by hemoglobin variants [ 19 ]. However, falsely low levels may occur in patients with hypoalbuminemia, for example, in patients with nephrotic syndrome or severe liver disease [ 29 ]. The glycated albumin test, reported as a percentage of total albumin, also reflects short-term glycemic status, typically over the preceding 2–3 weeks, and is not influenced by situations that falsely alter A1C levels [ 29 , 30 ]. Moreover, the tests that rely purely on blood glucose levels, including the oral glucose tolerance test (OGTT) and even continuous glucose monitoring, could possibly be the ones that are least affected by various factors, as discussed earlier. The OGTT is advocated for screening and diagnosis, and self-monitoring of blood glucose levels is advised for management during pregnancy [ 29 ]. Continuous glucose monitoring for up to 5 days has also been shown to correlate well with HbA1c levels [ 29 ].
The mutations associated with hemoglobin E disease are primarily seen to be prevalent in the eastern half of the Indian subcontinent and throughout Southeast Asia [ 12 , 23 ]. In 1954, Chernoff and colleagues first described that it has occurred in conjunction with β thalassemia, in which case it presents with a severe form of the disease known as the compound heterozygosity for hemoglobin E/β thalassemia [ 24 ], and since then several other cases have been reported from several parts of Southeast Asia [ 25 , 26 , 27 , 31 ]. Cases have been reported from some parts of Nepal, as well, but to our knowledge, this case report is the first ever report of an incidentally diagnosed HbE variant in a patient with type 2 diabetes mellitus in Nepal.
Several studies have evidenced and reported that various hemoglobinopathies, including HbE disease, interfere with accurate measurements of glycosylated hemoglobin, including HbA1c. A study conducted on the prevalence of hemoglobin variants and their effect on HbA1c measurement among the indigenous population of north Bengal showed Hb variants to have a significant effect on HbA1c measurement [ 32 ]. A clinically silent and very rare hemoglobinopathy, hemoglobin Himeji, has been reported in a Portuguese patient with diabetes with a discrepancy between fasting plasma glucose and HbA1c [ 33 ]. Yet another case series of two female Malay patients with HbJ, an Hb variant, showed persistently high HbA1c levels despite good glycemic control [ 34 ].
Because of the local occurrence of Hb variants and the ethnic origin of a given population, every individual laboratory must establish and validate its own assay method. Also, while managing patients with diabetes, knowledge of hemoglobinopathies influencing HbA1c determination methods is essential. Moreover, in populations with a high prevalence of hemoglobinopathies, hemoglobin typing should be considered basic information prior to HbA1c measurement, as suggested by some other studies, as well [ 35 ].
Hence, to conclude, clinicians should be aware of this limitation of HbA1c estimation by ion-exchange HPLC in patients with HbE and other Hb variants, though HPLC has been an important and one of the most commonly used modalities [ 26 ], among the several others such as immunoassay techniques, boronate affinity chromatography, etc., to detect it [ 18 ]. If the clinical impression and HbA1c test results do not match, then HbA1c values should be determined with a second method based on a different principle and confirmation of the glycemic status through alternative investigations. The boronate affinity method has been shown to be clinically reasonable for all hemoglobin variants. Similarly, the fructosamine test and the glycated albumin test could also be used as alternatives, as they are also not influenced by the presence of hemoglobin variants. The OGTT and continuous glucose monitoring can obviously be other reliable alternatives, though they have their own disadvantages, such as the fact that they will not reflect glycemic control over a longer period of time, as does the HbA1c, and need repeated measurements. Moreover, an abnormal HbA1c level in a diabetic patient or any other subject during routine evaluation or screening for diabetes could raise the suspicion of an Hb variant. Therefore, physicians and especially endocrinologists should take this fact into account and immediately seek further evaluation and investigations to confirm the diagnosis of Hb variants in such patients and advise the patients to screen their family members.
Availability of data and materials
Data and other materials can be made available if required.
Abbreviated Report of a WHO Consultation. Use of glycated haemoglobin (HbA1c) in the diagnosis of diabetes mellitus. 2011.
Campbell L, Pepper T, Shipman K. HbA1c: a review of non-glycaemic variables. J Clin Pathol. 2019;72(1):12–9.
Article CAS PubMed Google Scholar
UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837–53.
Article Google Scholar
Lim WY, et al . Screening for diabetes with HbA1c: test performance of HbA1c compared to fasting plasma glucose among Chinese, Malay and Indian community residents in Singapore. Sci Rep. 2018;8(1):12419.
Article PubMed PubMed Central Google Scholar
Nureslyna SI, et al . Percentage of haemoglobin variants detected during HbA1c analysis in hospital Kuala Lumpur. Malays J Med Health Sci. 2013;9(2):13–7.
Google Scholar
Schnedl WJ, et al . Evaluation of HbA1c determination methods in patients with hemoglobinopathies. Diabetes Care. 2000;23(3):339–44.
Chen Z, et al . Interpretation of HbA1c lies at the intersection of analytical methodology, clinical biochemistry and hematology (review). Exp Ther Med. 2022;24(6):707.
Article CAS PubMed PubMed Central Google Scholar
Bloomgarden Z, Handelsman Y. How does CKD affect HbA1c? J Diabetes. 2018;10(4):270.
Sehrawat T, et al . Utility and limitations of glycated hemoglobin (HbA1c) in patients with liver cirrhosis as compared with oral glucose tolerance test for diagnosis of diabetes. Diabetes Ther. 2018;9(1):243–51.
Lewis D, et al . Glycosylated haemoglobin in rheumatoid arthritis. Ann Rheum Dis. 1983;42(2):238–9.
Rhea JM, Molinaro R. Pathology consultation on HbA(1c) methods and interferences. Am J Clin Pathol. 2014;141(1):5–16.
Bachir D, Galacteros F. Hemoglobin E disease. Orphanet Encyclopedia. 2004.
Braunstein EM. Hemoglobin E disease. Merck Manual. 2017.
Fucharoen S, Weatherall DJ. The hemoglobin E thalassemias. Cold Spring Harb Perspect Med. 2012;2(8): a011734.
Eckfeldt JH, Bruns DE. Another step toward standardization of methods for measuring hemoglobin A1c. Clin Chem. 1997;43(10):1811–3.
Musalmah M, et al . Effect of hemoglobin E on glycosylated hemoglobin determinations using different commercial kits. Med J Malaysia. 2000;55(3):352–6.
CAS PubMed Google Scholar
Chen Y, et al . Influence and analysis of seven kinds of hemoglobin variants on HbA1c detection. Zhonghua Yixue Zazhi. 2014;94(6):438–41.
Little RR, Roberts WL. A review of variant hemoglobins interfering with hemoglobin A1c measurement. J Diabetes Sci Technol. 2009;3(3):446–51.
Paisooksantivatana K, et al . Influence of hemoglobin E on measurement of hemoglobin A1c by immunoassays. Diabetes Res Clin Pract. 2009;83(3):e84–5.
Guadalupe Vargas M, et al . Assessment of two glycated hemoglobin immunoassays. Endocrinol Diabetes Nutr (Engl Ed). 2020;67(5):297–303.
John WG, et al . Enzyme immunoassay—a new technique for estimating hemoglobin A1c. Clin Chem. 1993;39(4):663–6.
Watanabe T, et al . A nondiabetic case of hemoglobin variant (Hb Niigata) with inappropriately high and low HbA1c titers detected by different methods. Clin Chem. 1998;44(7):1562–4.
Weatherall DJ, Clegg JB. Inherited haemoglobin disorders: an increasing global health problem. Bull World Health Organ. 2001;79(8):704–12.
CAS PubMed PubMed Central Google Scholar
Chernoff AI, et al . Studies on hemoglobin E. I. The clinical, hematologic, and genetic characteristics of the hemoglobin E syndromes. J Lab Clin Med. 1956;47(3):455–89.
Minnich V, et al . Mediterranean anemia: a study of thirty-two cases in Thailand. Blood. 1954;9(1):1–23.
Yedla N, Kuchay MS, Mithal A. Hemoglobin E disease and glycosylated hemoglobin. Indian J Endocrinol Metab. 2015;19(5):683–5.
Olivieri NF, Pakbaz Z, Vichinsky E. Hb E/beta-thalassaemia: a common and clinically diverse disorder. Indian J Med Res. 2011;134(4):522–31.
Ribeiro RT, Macedo MP, Raposo JF. HbA1c, fructosamine, and glycated albumin in the detection of dysglycaemic conditions. Curr Diabetes Rev. 2016;12(1):14–9.
Mahabeer S. HbA1c measurement and assay interferences. Pathologists Lancet Laboratories, newsletter; 4th quarter. 2018.
Freitas PAC, Ehlert LR, Camargo JL. Glycated albumin: a potential biomarker in diabetes. Arch Endocrinol Metab. 2017;61(3):296–304.
Article PubMed Google Scholar
Premawardhena A, et al . Haemoglobin E beta thalassaemia in Sri Lanka. Lancet. 2005;366(9495):1467–70.
Roy S, et al . Prevalence of hemoglobin variants and their effect on Hba1c measurement among the indigenous population of north Bengal attending a tertiary care hospital. Asian J Med Sci. 2022;13(6):90–5.
Guedes V, et al . Hemoglobin Himeji and inconsistent hemoglobin A1c values: a case report. J Med Case Rep. 2017;11(1):201.
Wan Nik W, et al . Significantly high HbA(1c) in diabetic patient with Hb J: Case Report. Oman Med J. 2022;37(4): e393.
Mitchai M, et al . Misleading HbA1c measurement in diabetic patients with hemoglobin variants. Med Sci (Basel). 2021;9(2):43.
Download references
Acknowledgements
Not applicable.
Author information
Rashmi Karki, Samir Lamichhane, and Rekha Manandhar have contributed equally to this work.
Authors and Affiliations
National Public Health Laboratory (NPHL), Kathmandu, Nepal
Rashmi Karki, Runa Jha & Rekha Manandhar
Department of Clinical Pharmacology, Maharajgunj Medical Campus (MMC), Institute of Medicine (IOM), Tribhuvan University (TU), Kathmandu, Nepal
Samir Lamichhane
You can also search for this author in PubMed Google Scholar
Contributions
RK and RM conceptualized and designed the case report. The acquisition, analysis, and interpretation of patient data were also performed by RK and RM. The collection and assembly of relevant literature and background information, as well as writing and revising the manuscript focusing on the clinical aspects of the case, were done by SL. RK assisted SL in drafting and revising the manuscript, with a focus on the literature review. RK also contributed to the intellectual content and critical revision of the manuscript. Supervision and mentorship throughout the case report development were done by RJ and RM. All authors have read and approved the final version of the manuscript to be published.
Corresponding author
Correspondence to Samir Lamichhane .
Ethics declarations
Ethical approval and consent to participate.
Ethical approval from the institutional review board (IRB) has not been sought. Written informed consent was obtained from the patient for participation.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
Additional information, publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Karki, R., Lamichhane, S., Jha, R. et al. An incidental finding of a hemoglobin E variant in a diabetic patient with an abnormal glycated hemoglobin level: a case report. J Med Case Reports 18 , 279 (2024). https://doi.org/10.1186/s13256-024-04518-y
Download citation
Received : 06 December 2023
Accepted : 20 March 2024
Published : 15 June 2024
DOI : https://doi.org/10.1186/s13256-024-04518-y
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Hemoglobin E (HbE)
- Glycated hemoglobin (HbA1c)
Journal of Medical Case Reports
ISSN: 1752-1947
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
IMAGES
VIDEO
COMMENTS
The term presentation describes the leading part of the fetus or the anatomical structure closest to the maternal pelvic inlet during labor. The presentation can roughly be divided into the following classifications: cephalic, breech, shoulder, and compound. Cephalic presentation is the most common and can be further subclassified as vertex, sinciput, brow, face, and chin.
One such complication that can come at the last minute of any delivery is the presentation of the baby. Normally, babies bow down their chin well tucked into the chest during their journey through the birth canal. This position is called flexed position or vertex presentation. This is the ideal position that makes delivery easier as the baby ...
Brow presentation is a rare complication, which affects only one in every 500 to one in every 1,400 births. So the chances of it happening are low. If a brow presentation is picked up in early labour, your baby may still flex her head in time for the birth. Alternatively, she may tip her head further back and be born face first.
In the brow presentation, the occipitomental diameter, which is the largest diameter of the fetal head, is the presenting portion. Descent and internal rotation occur only with an adequate pelvis and if the face can fit under the pubic arch. While the head descends, it becomes wedged into the hollow of the sacrum. ...
Brow Presentation: Definition: Brow presentation occurs when the baby's head is partially extended, causing the brow (forehead) to lead the way through the birth canal. Causes: Brow presentation may result from abnormal fetal positioning, poor engagement of the fetal head, or other factors that prevent full flexion or extension.
In face presentation, the baby's neck arches back so that the face presents first rather than the top of the head.. In brow presentation, the neck is moderately arched so that the brow presents first.. Usually, fetuses do not stay in a face or brow presentation. These presentations often change to a vertex (top of the head) presentation before or during labor.
The vast majority of fetuses at term are in cephalic presentation. Approximately 5 percent of these fetuses are in a cephalic malpresentation, such as occiput posterior or transverse, face ( figure 1A-B ), or brow ( figure 2) [ 1 ]. Diagnosis and management of face and brow presentations will be reviewed here.
Toward the end of pregnancy, the fetus moves into position for delivery. Normally, the presentation is vertex (head first), and the position is occiput anterior (facing toward the pregnant patient's spine) with the face and body angled to one side and the neck flexed. Abnormal presentations include face, brow, breech, and shoulder.
7.10.1 Diagnosis. 7.10.2 Management. Foetus alive. Foetus dead. Brow presentation constitutes an absolute foeto-pelvic disproportion, and vaginal delivery is impossible (except with preterm birth or extremely low birth weight). This is an obstetric emergency, because labour is obstructed and there is a risk of uterine rupture and foetal distress.
Brow presentation is considered the rarest of all malpresentation with a prevalence of 1 in 500 to 1 in 4000 deliveries. Both face and brow presentations occur due to extension of the fetal neck instead of flexion; therefore, conditions that would lead to hyperextension or prevent flexion of the fetal neck can all contribute to face or brow ...
Brow Presentation: Brow is a cephalic deflection malpresentation with the partially deflexed fetal head midway between complete flexion (vertex) and full extension (face) (Fig. 2 ). The frontal bone is the designated point for its position in maternal pelvis. On vaginal examination, the brow, orbits, and root of the nose are palpable.
Brow presentation is considered the rarest of all malpresentation with a prevalence of 1 in 500 to 1 in 4000 deliveries. Both face and brow presentations occur due to extension of the fetal neck instead of flexion; therefore, conditions that would lead to hyperextension or prevent flexion of the fetal neck can all contribute to face or brow ...
In face presentation, the mentum (chin) and mouth are palpable. Management considerations for face, brow, and compounds presentations are unique with compound presentations having higher rates of vaginal delivery and lower complications as compared to either brow or face presentations. For brow presentations, approximately 30-40% of brow ...
Pertinent etiologic factors encountered in a series of 156 patients with brow presentation, representing an incidence of 1 in 670 deliveries, include cephalopelvic disproportion and prematurity only. The brow prolongs the deceleration phase and the second stage and exaggerates the deleterious effects that other pertinent factors exert on the course of labor.
Brow positions. The fetal head stays between full extension and full flexion so that the biggest diameter (the mento-vertex) presents. Brow presentation occurs in 0.14% of deliveries 5. Brow presentation is usually only diagnosed once labour is well established. The anterior fontanelle and super orbital ridges are palpable on vaginal examination.
Definition — Brow presentation refers to a presentation in which the fetal surface presenting in the birth canal extends from the anterior fontanelle to the brow (orbital ridge), but does not include the mouth and chin . The fetal neck is extended, but not to the degree of a face presentation. ...
In Labor with a Face or Brow Presentation. Back baby up! Forward-leaning Inversion with a jiggle of the buttocks right through 1-2 contractions often backs baby up so they can tuck their chin. Then they can aim into the pelvis with an easier position. Shake the Apples in Forward-leaning Inversion with hands. A little effort can make labor a lot ...
In the brow presentation, the head is slightly extended, but less than in the face presentation. The chin presentation is a variant of the face presentation with maximum extension of the head. Non-cephalic presentations are the breech presentation (3.5%) and the shoulder presentation (0.5%). Vertex presentation
This may mean simple manual procedures to help reposition the baby or, in many cases, a planned C-section delivery. The failure of healthcare professionals to identify and quickly resolve issues related to fetal size, ... As the term "brow presentation" suggests, the brow (forehead) is the part that is situated to go through the pelvis ...
This is known as a brow presentation or forehead presentation. It is an extremely rare condition, occurring once in 1500 births. Brow presentation might obstruct vaginal births from occurring as there is less space for the baby to drop down towards the pelvic girdle. However, if brow presentation occurs early in labour, there is still time for ...
Cephalo pelvic disproportion has been associated with brow presentation in from 7.7 to 53.8 per cent of cases,l' 8-12, 15, 19, 20 but the impor-tance of this factor has been doubted by some.21, 22 Leiomyomas of the uterus10, 19 and bicornuate uterus19 have been reported to be associated with the abnormal presentation.
brow presentation: presentation of any part of the fetal head, usually the upper and back part, as a result of flexion such that the chin is in contact with the thorax in vertex presentation; there may be degrees of flexion so that the presenting part is the large fontanel in sincipital presentation, the brow in brow presentation, or the face ...
For those looking for the hidden hand of politics in what the Supreme Court does, there's plenty of reason for suspicion on Donald Trump's as-yet-undecided immunity case given its urgency.
Explore the significance of Juneteenth and the value of making it a national holiday
Glycated hemoglobin (HbA1c), initially identified as "unusual" hemoglobin in patients with diabetes over half a century ago [], has now become a well-known marker of long-term glycemic control in individuals with diabetes mellitus [], reflecting an average blood glucose level over a period of around 3 months.Glycemic control being an important factor for the progression to long-term ...