
Assignment of benefit and signature requirements for MBS telehealth services
Update from Minister Butler - 6/10/23 Following the RACGP’s representations to Minister Butler, the Minister has advised that he has asked his department to provide options to address concerns about the assignment of benefit for Medicare bulk billed claims, including legislative amendments. The department has informed the Minister that until these changes are made, there are no plans to pursue any broad punitive actions on this issue unless it relates to fraudulent claims against Medicare.
The new assignment of benefit process outlined below remains in effect. The RACGP will provide further updates on this issue in due course.
GPs now need to document verbal consent from bulk billed telehealth patients using an approved form which can be downloaded from the Services Australia website . Previously the Department of Health and Aged Care (DoHAC) said verbal consent for telehealth consultations could be documented in a patient’s clinical notes, but this is no longer the case.
When seeking verbal consent for telehealth services:
- DB4E digital form for electronically transmitted claims that can be claimed through HPOS Bulk Bill Webclaim. In most scenarios a DB4E is the appropriate form to use.
- DB020 digital form to be used with Medicare Bulk Bill Webclaims.
- Obtain verbal consent and explain to the patient how you will document their agreement.
- If the patient agrees, type ‘ patient verbally agreed ’ in the signature field.
- Provide a copy of the form to the patient, ideally by email or text for record keeping.
- Keep a copy of all claims and forms for at least two years. This is for auditing purposes if you are subject to a compliance review.
More information about the new assignment of benefit and signature requirements for Medicare Benefits Schedule (MBS) telehealth services is available on the Services Australia website .
DoHAC have published frequently asked questions for providers on the new requirements, which are available from MBS Online .
What is the assignment of benefit rule?
The requirement for a patient’s signature is considered an important deterrent to fraud (eg claims for services that were not provided). The DoHAC is obligated to enforce these rules under section 20A of the Health Insurance Act 1973.
Compliance and auditing
We have received assurances from the DoHAC that no retrospective compliance activities will be completed. However, it is unclear what compliance measures will be undertaken going forward, so we strongly encourage members to follow the correct processes when providing bulk billed telehealth services. You should keep a copy of all correspondence, claims and forms for at least two years for auditing purposes.
RACGP advocacy: cut the red tape
We know many members see this change as further red tape, and a potential barrier to providing bulk billed care, and we are advocating for a better solution.
The RACGP considers the need to document consent using a form to be an antiquated requirement that must be urgently reviewed. We will be raising our concerns with the Health Minister and calling for a solution that reflects current workflows in general practice.
Our preference is for verbal consent to remain available for bulk billed telehealth consultations, with a digital solution to record consent which minimises the administrative impact on GPs and practice teams. The digital solution needs to be fully integrated with existing clinical information systems and data so it easily fits in with clinical workflows.
Stay up to date with our advocacy on this issue. We know this is frustrating, and we invite you to share your feedback or questions with us. Please email [email protected] to get in touch and let us know if the RACGP can share your de-identified feedback with the DoHAC. Write to your local MP
RACGP members can write to their local federal MP about changes to assignment of benefit rules using the letter template below. The document has editable fields for you to fill in before sending. Click here to find details of your local MP. You can search by name, postcode or electorate. Download the letter template.
Advertising
Does your provider accept Medicare as full payment?
You can get the lowest cost if your doctor or other health care provider accepts the Medicare-approved amount as full payment for a covered service. This is called “accepting assignment.” If a provider accepts assignment, it’s for all Medicare-covered Part A and Part B services.
Using a provider that accepts assignment
Most doctors, providers, and suppliers accept assignment, but always check to make sure that yours do.
If your doctor, provider, or supplier accepts assignment:
- Your out-of-pocket costs may be less.
- They agree to charge you only the Medicare deductible and coinsurance amount, and usually wait for Medicare to pay its share before asking you to pay your share.
- They have to submit your claim directly to Medicare and can't charge you for submitting the claim.
How does assignment impact my drug coverage?
Using a provider that doesn't accept Medicare as full payment
Some providers who don’t accept assignment still choose to accept the Medicare-approved amount for services on a case-by-case basis. These providers are called "non-participating."
If your doctor, provider, or supplier doesn't accept assignment:
- You might have to pay the full amount at the time of service.
- They should submit a claim to Medicare for any Medicare-covered services they give you, and they can’t charge you for submitting a claim. If they refuse to submit a Medicare claim, you can submit your own claim to Medicare. Get the Medicare claim form .
- They can charge up to 15% over the Medicare-approved amount for a service, but no more than that. This is called "the limiting charge."
Does the limiting charge apply to all Medicare-covered services?
Using a provider that "opts-out" of Medicare
- Doctors and other providers who don’t want to work with the Medicare program may "opt out" of Medicare.
- Medicare won’t pay for items or services you get from provider that opts out, except in emergencies.
- Providers opt out for a minimum of 2 years. Every 2 years, the provider can choose to keep their opt-out status, accept Medicare-approved amounts on a case-by-case basis ("non-participating"), or accept assignment.
Find providers that opted out of Medicare.
Private contracts with doctors or providers who opt out
- If you choose to get services from an opt-out doctor or provider you may need to pay upfront, or set up a payment plan with the provider through a private contract.
- Medicare won’t pay for any service you get from this doctor, even if it’s a Medicare-covered service.
What are the rules for private contracts?
You may want to contact your State Health Insurance Assistance Program (SHIP) for help before signing a private contract with any doctor or other health care provider.
What do you want to do next?
- Next step: Get help with costs
- Take action: Find a provider
- Get details: How to get Medicare services
- Type 2 Diabetes
- Heart Disease
- Digestive Health
- Multiple Sclerosis
- COVID-19 Vaccines
- Occupational Therapy
- Healthy Aging
- Health Insurance
- Public Health
- Patient Rights
- Caregivers & Loved Ones
- End of Life Concerns
- Health News
- Thyroid Test Analyzer
- Doctor Discussion Guides
- Hemoglobin A1c Test Analyzer
- Lipid Test Analyzer
- Complete Blood Count (CBC) Analyzer
- What to Buy
- Editorial Process
- Meet Our Medical Expert Board
Medicare Assignment: Everything You Need to Know
Medicare assignment.
- Providers Accepting Assignment
- Providers Who Do Not
- Billing Options
- Assignment of Benefits
- How to Choose
Frequently Asked Questions
Medicare assignment is an agreement between Medicare and medical providers (doctors, hospitals, medical equipment suppliers, etc.) in which the provider agrees to accept Medicare’s fee schedule as payment in full when Medicare patients are treated.
This article will explain how Medicare assignment works, and what you need to know in order to ensure that you won’t receive unexpected bills.
fizkes / Getty Images
There are 35 million Americans who have Original Medicare. Medicare is a federal program and most medical providers throughout the country accept assignment with Medicare. As a result, these enrollees have a lot more options for medical providers than most of the rest of the population.
They can see any provider who accepts assignment, anywhere in the country. They can be assured that they will only have to pay their expected Medicare cost-sharing (deductible and coinsurance, some or all of which may be paid by a Medigap plan , Medicaid, or supplemental coverage provided by an employer or former employer).
It’s important to note here that the rules are different for the 29 million Americans who have Medicare Advantage plans. These beneficiaries cannot simply use any medical provider who accepts Medicare assignment.
Instead, each Medicare Advantage plan has its own network of providers —much like the health insurance plans that many Americans are accustomed to obtaining from employers or purchasing in the exchange/marketplace .
A provider who accepts assignment with Medicare may or may not be in-network with some or all of the Medicare Advantage plans that offer coverage in a given area. Some Medicare Advantage plans— health maintenance organizations (HMOs) , in particular—will only cover an enrollee’s claims if they use providers who are in the plan's network.
Other Medicare Advantage plans— preferred provider organizations (PPOs) , in particular—will cover out-of-network care but the enrollee will pay more than they would have paid had they seen an in-network provider.
Original Medicare
The bottom line is that Medicare assignment only determines provider accessibility and costs for people who have Original Medicare. People with Medicare Advantage need to understand their own plan’s provider network and coverage rules.
When discussing Medicare assignment and access to providers in this article, keep in mind that it is referring to people who have Original Medicare.
How to Make Sure Your Provider Accepts Assignment
Most doctors, hospitals, and other medical providers in the United States do accept Medicare assignment.
Provider Participation Stats
According to the Centers for Medicare and Medicaid Services, 98% of providers participate in Medicare, which means they accept assignment.
You can ask the provider directly about their participation with Medicare. But Medicare also has a tool that you can use to find participating doctors, hospitals, home health care services, and other providers.
There’s a filter on that tool labeled “Medicare-approved payment.” If you turn on that filter, you will only see providers who accept Medicare assignment. Under each provider’s information, it will say “Charges the Medicare-approved amount (so you pay less out-of-pocket).”
What If Your Provider Doesn’t Accept Assignment?
If your medical provider or equipment supplier doesn’t accept assignment, it means they haven’t agreed to accept Medicare’s approved amounts as payment in full for all of the services.
These providers can still choose to accept assignment on a case-by-case basis. But because they haven’t agreed to accept Medicare assignment for all services, they are considered nonparticipating providers.
Note that "nonparticipating" does not mean that a provider has opted out of Medicare altogether. Medicare will still pay claims for services received from a nonparticipating provider (i.e., one who does not accept Medicare assignment), whereas Medicare does not cover any of the cost of services obtained from a provider who has officially opted out of Medicare.
If a Medicare beneficiary uses a provider who has opted out of Medicare, that person will pay the provider directly and Medicare will not be involved in any way.
Physicians Who Have Opted Out
Only about 1% of all non-pediatric physicians have opted out of Medicare.
For providers who have not opted out of Medicare but who also don’t accept assignment, Medicare will still pay nearly as much as it would have paid if you had used a provider who accepts assignment. Here’s how it works:
- Medicare will pay the provider 95% of the amount they would pay if the provider accepted assignment.
- The provider can charge the person receiving care more than the Medicare-approved amount, but only up to 15% more (some states limit this further). This extra amount, which the patient has to pay out-of-pocket, is known as the limiting charge . But the 15% cap does not apply to medical equipment suppliers; if they do not accept assignment with Medicare, there is no limit on how much they can charge the person receiving care. This is why it’s particularly important to make sure that the supplier accepts Medicare assignment if you need medical equipment.
- The nonparticipating provider may require the person receiving care to pay the entire bill up front and seek reimbursement from Medicare (using Form CMS 1490-S ). Alternatively, they may submit a claim to Medicare on behalf of the person receiving care (using Form CMS-1500 ).
- A nonparticipating provider can choose to accept assignment on a case-by-case basis. They can indicate this on Form CMS-1500 in box 27. The vast majority of nonparticipating providers who bill Medicare choose to accept assignment for the claim being billed.
- Nonparticipating providers do not have to bill your Medigap plan on your behalf.
Billing Options for Providers Who Accept Medicare
When a medical provider accepts assignment with Medicare, part of the agreement is that they will submit bills to Medicare on behalf of the person receiving care. So if you only see providers who accept assignment, you will never need to submit your own bills to Medicare for reimbursement.
If you have a Medigap plan that supplements your Original Medicare coverage, you should present the Medigap coverage information to the provider at the time of service. Medicare will forward the claim information to your Medigap insurer, reducing administrative work on your part.
Depending on the Medigap plan you have, the services that you receive, and the amount you’ve already spent in out-of-pocket costs, the Medigap plan may pay some or all of the out-of-pocket costs that you would otherwise have after Medicare pays its share.
(Note that if you have a type of Medigap plan called Medicare SELECT, you will have to stay within the plan’s network of providers in order to receive benefits. But this is not the case with other Medigap plans.)
After the claim is processed, you’ll be able to see details in your MyMedicare.gov account . Medicare will also send you a Medicare Summary Notice. This is Medicare’s version of an explanation of benefits (EOB) , which is sent out every three months.
If you have a Medigap plan, it should also send you an EOB or something similar, explaining the claim and whether the policy paid any part of it.
What Is Medicare Assignment of Benefits?
For Medicare beneficiaries, assignment of benefits means that the person receiving care agrees to allow a nonparticipating provider to bill Medicare directly (as opposed to having the person receiving care pay the bill up front and seek reimbursement from Medicare). Assignment of benefits is authorized by the person receiving care in Box 13 of Form CMS-1500 .
If the person receiving care refuses to assign benefits, Medicare can only reimburse the person receiving care instead of paying the nonparticipating provider directly.
Things to Consider Before Choosing a Provider
If you’re enrolled in Original Medicare, you have a wide range of options in terms of the providers you can use—far more than most other Americans. In most cases, your preferred doctor and other medical providers will accept assignment with Medicare, keeping your out-of-pocket costs lower than they would otherwise be, and reducing administrative hassle.
There may be circumstances, however, when the best option is a nonparticipating provider or even a provider who has opted out of Medicare altogether. If you choose one of these options, be sure you discuss the details with the provider before proceeding with the treatment.
You’ll want to understand how much is going to be billed and whether the provider will bill Medicare on your behalf if you agree to assign benefits (note that this is not possible if the provider has opted out of Medicare).
If you have supplemental coverage, you’ll also want to check with that plan to see whether it will still pick up some of the cost and, if so, how much you should expect to pay out of your own pocket.
A medical provider who accepts Medicare assignment is considered a participating provider. These providers have agreed to accept Medicare’s fee schedule as payment in full for services they provide to Medicare beneficiaries. Most doctors, hospitals, and other medical providers do accept Medicare assignment.
Nonparticipating providers are those who have not signed an agreement with Medicare to accept Medicare’s rates as payment in full. However, they can agree to accept assignment on a case-by-case basis, as long as they haven’t opted out of Medicare altogether. If they do not accept assignment, they can bill the patient up to 15% more than the Medicare-approved rate.
Providers who opt out of Medicare cannot bill Medicare and Medicare will not pay them or reimburse beneficiaries for their services. But there is no limit on how much they can bill for their services.
A Word From Verywell
It’s in your best interest to choose a provider who accepts Medicare assignment. This will keep your costs as low as possible, streamline the billing and claims process, and ensure that your Medigap plan picks up its share of the costs.
If you feel like you need help navigating the provider options or seeking care from a provider who doesn’t accept assignment, the Medicare State Health Insurance Assistance Program (SHIP) in your state may be able to help.
A doctor who does not accept Medicare assignment has not agreed to accept Medicare’s fee schedule as payment in full for their services. These doctors are considered nonparticipating with Medicare and can bill Medicare beneficiaries up to 15% more than the Medicare-approved amount.
They also have the option to accept assignment (i.e., accept Medicare’s rate as payment in full) on a case-by-case basis.
There are certain circumstances in which a provider is required by law to accept assignment. This includes situations in which the person receiving care has both Medicare and Medicaid. And it also applies to certain medical services, including lab tests, ambulance services, and drugs that are covered under Medicare Part B (as opposed to Part D).
In 2021, 98% of American physicians had participation agreements with Medicare, leaving only about 2% who did not accept assignment (either as a nonparticipating provider, or a provider who had opted out of Medicare altogether).
Accepting assignment is something that the medical provider does, whereas assignment of benefits is something that the patient (the Medicare beneficiary) does. To accept assignment means that the medical provider has agreed to accept Medicare’s approved fee as payment in full for services they provide.
Assignment of benefits means that the person receiving care agrees to allow a medical provider to bill Medicare directly, as opposed to having the person receiving care pay the provider and then seek reimbursement from Medicare.
Centers for Medicare and Medicaid Services. Medicare monthly enrollment .
Centers for Medicare and Medicaid Services. Annual Medicare participation announcement .
Centers for Medicare and Medicaid Services. Lower costs with assignment .
Centers for Medicare and Medicaid Services. Find providers who have opted out of Medicare .
Kaiser Family Foundation. How many physicians have opted-out of the Medicare program ?
Center for Medicare Advocacy. Durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) updates .
Centers for Medicare and Medicaid Services. Check the status of a claim .
Centers for Medicare and Medicaid Services. Medicare claims processing manual. Chapter 26 - completing and processing form CMS-1500 data set .
Centers for Medicare and Medicaid Services. Ambulance fee schedule .
Centers for Medicare and Medicaid Services. Prescription drugs (outpatient) .
By Louise Norris Norris is a licensed health insurance agent, book author, and freelance writer. She graduated magna cum laude from Colorado State University.
Medicare Benefits Schedule
- Create publication
- Fact Sheets
- MBS interpretation
Medicare Benefits Schedule - Note PN.2.2
Search Results for Note PN.2.2
Category 6 - PATHOLOGY SERVICES
Responsibilities of Approved Pathology Practitioners
Form of Request
There is no official "request in writing" form, and the requesting practitioner's own stationery, or pre-printed forms supplied by Approved Pathology Practitioners/Authorities are acceptable.
For the purposes of Medicare eligible services, the minimum information requirements for a pre-printed pathology request and combined pathology request/offer to assign are detailed within the: Health Insurance Act 1973 ; Health Insurance Regulations 2018 ; and the Privacy Act 1988 .
The following table presents the minimum details that pre-printed pathology request forms and combined pathology request/offer to assign forms must contain for the purposes of a subsequent Medicare claim:
Services Australia has developed a Health Practitioner Guideline to substantiate that a valid request existed (pathology or diagnostic imaging) which is located on the Services Australia website.
An Approved Pathology Practitioner or Approved Pathology Authority who, without reasonable excuse, provides to practitioners (directly or indirectly) combined request/assignment forms which are not in accordance with the legislation is guilty of an offence under the Health Insurance Act 1973 punishable, upon conviction, by a fine not exceeding 10 Penalty Units (in accordance with the Crimes Act 1914 ).
Patient Copy
Assignment of benefits requires the patient to receive a copy of the request. The doctor must cause the particulars relating to the professional service (tests requested) to be set out on the assignment form, before the patient signs the form and cause the patient to receive a copy of the form as soon as practicable after the patient signs it.
Authority to lodge a Patient Claim electronically
Where an Approved Pathology Practitioner or Approved Pathology Authority renders a service and the patient has not assigned the benefit the Approved Pathology Practitioner or Approved Pathology Authority can lodge a claim electronically to Services Australia on behalf of the patient where consent is provided. This consent can be provided verbally.
Combined Online Patient Claiming Authority
Authority for APP/APA to submit an electronic patient claim on behalf of the claimant
An example of wording that could be used is: 'I authorise the approved pathology practitioner who will render the requested pathology services, and any further pathology services which the practitioner determines to be necessary, to submit my unpaid account to Medicare, so that Medicare can assess my claim and issue me a cheque made payable to the practitioner, for the Medicare benefit.'
Patient Signature___________________ Date______/______/_______
Verbal consent was provided by patient to submit unpaid account to Medicare. No signature available .
Request to Approved Pathology Authority
It is acceptable for a request to be made to an Approved Pathology Authority who is the proprietor or one of the proprietors of a laboratory instead of making the request to the Approved Pathology Practitioner who renders the service or on whose behalf the service is rendered.
Holding, Retention, Recording and Production of Request Forms
Approved Pathology Practitioners must hold a request in writing for all services requested by any other practitioner before billing patients. An Approved Pathology Practitioner is required to retain written requests/confirmation of requests for pathology services for 2 years from the day when the service was rendered. This also applies to requests which an Approved Pathology Practitioner receives of which only some tests are referred to another Approved Pathology Practitioner (the first Approved Pathology Practitioner would retain the request for 2 years). If all tests were referred, the second pathologist would retain the original request.
If the written request or written confirmation has been recorded on film or other magnetic medium approved by the Minister for Health and Aged Care, for the purposes of storage and subsequent retrieval, the record so made shall be deemed to be a retention of the request or confirmation. The production or reproduction of such a record shall be deemed to be a production of the written request or written confirmation.
An Approved Pathology Practitioner or an Approved Pathology Authority is required to produce, on request from the Services Australia CEO, no later than the end of the day following the request from the CEO, a written request or written confirmation retained pursuant to the above paragraphs. An employee of Services Australia is authorised to make and retain copies of or take and retain extracts from written requests or written confirmations.
Offences in Relation to Retaining and Producing Request Forms
The following offences are punishable upon conviction by a fine not exceeding 10 penalty units:
- an Approved Pathology Practitioner who, without reasonable excuse, does not keep request forms for 2 years;
- an Approved Pathology Practitioner who, without reasonable excuse, does not produce a request form to an employee of Services Australia before the end of the day following the day of Services Australia CEO's request;
- an Approved Pathology Authority which, without reasonable excuse, does not keep request forms for 2 years;
- an Approved Pathology Authority which, without reasonable excuse, does not produce a request form to an employee of the Services Australia before the end of the day following the day of Services Australia CEO's request.
Referral From An Approved Pathology Practitioner To Another Approved Pathology Practitioner
Where an Approved Pathology Practitioner refers some or all services requested to another Approved Pathology Practitioner not associated with the same Approved Pathology Authority the following apply:
- where all the services are referred, the first Approved Pathology Practitioner should forward the original request to the second Approved Pathology Practitioner, and the document bearing the patient's assignment voucher so that the second Approved Pathology Authority can direct-bill Medicare;
- name and provider number of the original requesting practitioner; and
- date of original request;
- under the item coning rules (which limit benefits for multiple services) only one Medicare benefit is payable for services included in coned items except for estimations covered by Rule 6 entitled "designated pathology services". The exemption allows payment of more than one Medicare benefit where various components of the one item number from the same request e.g. drug assays (items 66800 and 66812) are performed by two Approved Pathology Authorities.
Although the provisions concerning designated pathology services in Rule 6 permit similar services (e.g. hormone estimations) to be performed by 2 or more laboratories, with different Approved Pathology Authorities, the sum of the Medicare benefit payable for services provided by the laboratories concerned will not exceed the maximum amount payable under the item coning rules when a single laboratory performs all the estimations.
- the patient should be billed by each Approved Pathology Practitioner only for those services rendered by or on his/her behalf;
- photocopies of requests are not acceptable;
- in the case of "designated pathology services" 65150, 65175, 66650, 66695, 66711, 66722, 66785, 66800,66812, 66819, 66825, 69384, 69494, 71089, 71153 or 71165 a patient episode initiation fee (PEI) is payable for the services provided by the laboratory which receives the original request and performs one or more of the estimations. However, no PEI is payable for services provided by the other laboratory which performs the remainder of the estimations. A "specimen referred fee" is payable instead. One Approved Pathology Practitioner cannot claim both a PEI and a "specimen referred fee" in relation to the same patient episode.
Offence Not To Confirm An Oral Request
An Approved Pathology Practitioner who, without reasonable excuse, does not confirm in writing an oral request to another Approved Pathology Practitioner within fourteen days of making the oral request is guilty of an offence under the Health Insurance Act 1973 punishable, upon conviction, by a fine not exceeding 10 Penalty Units (in accordance with the Crimes Act 1914 ), and the request is deemed never to have been made.
- Previous - Note PN.2.1
- Next - Note PN.2.3
- Assist - Addition/Deletion of (Assist.)
- Amend - Amended Description
- Anaes - Anaesthetic Values Amended
- Emsn - EMSN Change
- Fee - Fee Amended
- Renum - Item Number Change (renumbered)
- New - New Item
- NewMin - New Item (previous Ministerial Determination)
- Qfe - QFE Change
© Commonwealth of Australia ABN: 83 605 426 759
- Accessibility
About the MBS
- Book Appointment
Medicare and Digital Signing of DB4 Benefit Assignment Forms
The executive summary is that GP2U now offers Australia's only Medicare approved digital signing of DB4 form process. With a couple of mouse clicks a patient can now legally assign their Medicare benefits to a remotely located specialist. The background to this ground breaking eHealth development is presented below.
What section 20A says is that a patient can assign their Medicare benefit to their treating doctor by signing the approved form, where the approved form is the form approved in writing by the minister. The approved form is called a DB4 form .
With the advent of Telehealth a problem arises. How does a Specialist obtain the signature of a patient who is not in the same physical location? The initial Medicare advice to doctors was that a patient's verbal consent over a video conference link would be accepted as satisfactory for the purposes of Section 20A and the assignment of patient Medicare benefits. Earlier this year that advice was revoked and replaced with advice that doctors could either get a physical signature using paper DB4 forms and regular mail, or use an email process.
At GP2U our core focus is on making Telehealth easy. Sending physical DB4 forms by ordinary mail, or using a complicated email process, that, like verbal assignment of benefits process that preceded it appears non compliant with the requirements of section 20A, seemed to be making Telehealth harder - so we started thinking.....
The Electronic Transactions Act (1999) sets out the requirements for a digital signature. The GP2U process for a digital signature follows the industry standard MD5/RSA algorithm as specified by the World Wide Web Consortium (W3C). W3C is the peak organisation largely responsible for Internet standards. The detailed W3C technical specification for a digital signature is found here .
" In relation to the digitally signed DB4 it appears, based on the information you have provided, that your model would meet the requirements of the Health Insurance Act 1975 (the HIA) for the assignment of Medicare benefits"
You can read the full text of the Medicare approval letter here .
Please be aware that as of 26 March 2020 only Telehealth appointments can be made via our online booking service. To make a telehealth booking click on BOOK NOW
At the time of your appointment please leave your phone free to accept your doctors incoming video or voice call.
If you would like a face to face appointment at the clinic please call our friendly reception staff on 9781 3300
Introducing Assignment of Benefit Via SMS message
Bulk billing (or direct billing) is where a medical practitioner, with the patient’s agreement, accepts the patient’s Medicare benefit as full payment for a service. When a practitioner bulk bills a patient, the practitioner can receive the Medicare benefit for the service directly from Services Australia, using the online claiming facility.
Section 20A of the Act provides for bulk billing. For an assignment of benefit in accordance with Section 20A, there must be an agreement under which the patient (or person responsible for the medical expenses such as a parent of a patient) assigns their right to a Medicare benefit to the practitioner who must accept it as ‘full payment of the medical expenses incurred in respect of the professional service’ provided.
A patient is required to sign a Medicare assignment of benefit form for a bulk-billed professional service, unless using an online system such as Medicare Easyclaim or any other system that allows the patient to digitally sign an electronic assignment. The patient must be offered a digital or paper copy of the assignment of benefit form to retain.
The assignment of Medicare Benefits is NOT a new process. It has been mandated from the inception of Medicare, many years ago.
The Department allowed clinics to obtain verbal agreement for the assignment of their Medicare Benefit for Telehealth as an interim measure during COVID. This dead-line was set for the end of 2022.
This deadline has been extended, with no confirmation as yet of a new dead-line at time of writing.
The assignment of Medicare Benefits applies to ALL Bulk Billed consults, both in-clinic and Telehealth.
The assignment of Medicare Benefits does NOT apply to private billing.
Patients receive a secure SMS from the clinic’s dedicated AutoMed Message gateway.
The message will always be delivered from a dedicated mobile number that has been assigned to the clinic, which assists in building confidence that the message is secure and from a known source.
The message will look like this:
Patients need to enter their Date-Of-Birth as recorded in the Clinic’s PMS (Practice Management Software) to access the information relating to their bulk-billed consult.
The format required is displayed within the message i.e. ddmmyyyy
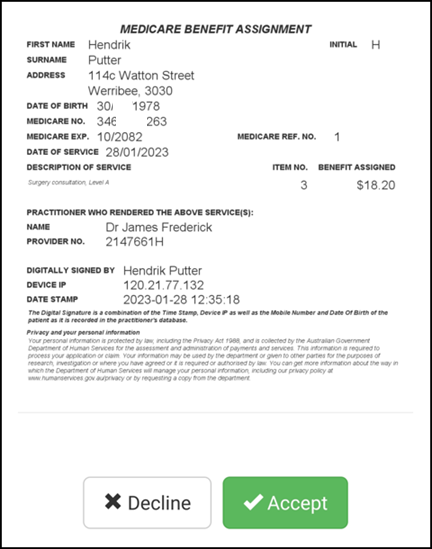
Then click ACCEPT
- Testimonials
- Accommodation
- Transcription
Spinal Surgery Medical Claims Payment Integrity Report
- Medicare PhD Thesis
- Sign Up Now
- Client Log-in
Home > News > COVID MBS items FAQs No.14, 31 March 2020, Special Edition Bulk Bill Signature Explainer

Dear Doctors and Health Care Workers
Following on from yesterday’s bulletin, as promised, this is an explainer on the law around the requirement for patients to sign the Bulk Bill voucher, known as the DB4 form.
As an academic scholar of Medicare law, bulk billing strikes at the heart of my doctorate and is something I have written about here https://www.ncbi.nlm.nih.gov/pubmed/31682343 , and in “Australian Doctor” here https://www.ausdoc.com.au/workwise/youre-likely-guilty-so-beware-law-trumps-medicare-advice-bulk-bill-vouchers . I have also spoken about it on the RACP Pomegranate Health podcast here https://podcasts.apple.com/gb/podcast/ep56-billing-in-byzantium/id1022747864?i=1000468184705 and have even written a short course on it here https://www.aimactraining.com/shop/product/bulk-billing-medicares-heart-beat .
Bulk billing is Medicare’s heartbeat, yet it is one of the most poorly understood areas of Medicare billing. So, I’m going to be succinct and as clear as I can to see if we can put this issue to bed. I will underline key words and phrases to guide you through.
First the Law
Section 20A(1) of the Health Insurance Act (the Act) https://www.legislation.gov.au/Details/C2020C00063 describes the bulk billing process. Here it is:
“20A Assignment of Medicare benefit
(1) Where a medicare benefit is payable to an eligible person in respect of a professional service rendered to the eligible person or to another eligible person, the first‑mentioned eligible person and the person by whom, or on whose behalf, the professional service is rendered (in this subsection referred to as the practitioner ) may enter into an agreement, in accordance with the approved form, under which:
(a) the first‑mentioned eligible person assigns his or her right to the payment of the medicare benefit to the practitioner; and
(b) the practitioner accepts the assignment in full payment of the medical expenses incurred in respect of the professional service by the first‑mentioned eligible person.”
Section 20B(3) of the Act describes the method by which the patient assigns their Medicare benefit. This is done by the patient signing the assignment of benefit form. Here is section 20B(3) with the word ‘signed’ underlined for you.
“(3) A claim referred to in subsection (2) shall not be paid unless the claimant satisfies the Chief Executive Medicare that:
(c) in the case of an agreement under subsection 20A(1) that was signed by each party in the presence of the other—the assignor retained in his or her possession after the agreement was so signed a copy of the agreement;”
TO SUMMARISE: This legal requirement has existed since the scheme was first introduced as Medibank in 1975. Yes, that far back. And it has never changed. So, to be absolutely clear – there has always been a legal requirement for patients to sign bulk bill forms to evidence consent. Always .
What has the High Court said about this?
In the High Court case of Wong v Commonwealth of Australia; Selim v Lele, Tan and Rivett constituting the Professional Services Review Committee No 309 [2009] HCA 3 (2 February 2009) the bulk bill consent requirement was described in the following terms:
“Even “bulk billing” is only possible by consent of both parties to that relationship. In these ways, the legislation avoids impermissible forms of “civil conscription” which the grant of power was thought otherwise possibly to entail.”
Why it matters
The patient’s signature on the Medicare assignment form is important for two reasons:
- It is the only active involvement the patient has in a bulk billing transaction, and it therefore provides the only opportunity for the patient to review the services being claimed against her/his Medicare number, and
- It is a critically important safeguard against fraudulent billing (such as billing for fictitious attendances) because it is the only evidence of both the practitioner and patient being in the same place at the same time.
So how on earth did we all get it so wrong for so long?
Because of this content on Medicare’s website.
“Assignment of benefit documents
Assignment of benefit forms no longer need to be stored at the practice if you are using Medicare Online.”
Here’s the link https://www.servicesaustralia.gov.au/organisations/health-professionals/services/medicare/medicare-online-health-professionals (accessed today)
This happened about 10 years ago, when in one fell swoop, the department undid a critically important tenet of the Medicare scheme, rendering it more vulnerable to abuse, because pretty much the entire country stopped asking patients to sign bulk bill forms once Medicare adopted this position.
I mean, why print a piece of paper and have the patient sign it and then be permitted to bin it!
Putting all this in COVID context
The underlying sections of the law have not changed. Section 20A and 20B remain in force.
Further, these important machinery provisions of the Medicare scheme are unlikely to ever be changed because it would require a parliamentary process, which would be unlikely to succeed because it would be just too damaging to the scheme.
So, the department is currently approaching this issue via informal channels, which is appropriate given the current circumstances.
They are sending emails and asking they be widely disseminated to all stakeholders stating their position on the bulk bill signature issue. We receive these emails, and I’m sure many of you do also. The most recent departmental email we copied and pasted for you in Bulletin 9 at point 6 https://synapsemedical.com.au/news/2020/03/26/covid-mbs-items-explainer-and-faqs-no-9-26-march-2020/
In summary, the department has relaxed the above requirements for COVID items only and stated they will not conduct audits of this requirement during this period. They have given 3 options for consent which are: in writing, by email or verbally through the video/phone link. They have also said consent can be provided by another person such as another family member or carer and have suggested a note be made in the medical record that the patient consented to assign their benefit to the practitioner.
This is all very sensible and helpful during this difficult period.
Other important ongoing legal provisions relating to bulk billing
- Asking patients to sign blank bulk bill forms or forms with missing details is illegal (see section 127 of the Act)
- Not giving patients a copy of their signed bulk bill form is an offence, but penalties can be waived if you have a ‘reasonable excuse’ why you didn’t give it to the patient. One might be – the patient didn’t want it.
- Using a Medicare Ezyclaim terminal has a special legal provision, so having the patient (not you) press ‘yes’ on the terminal is a legally valid signature
- If the patient is unable to sign, you can indicate ‘unable to sign’ and notate why. This has always been available.
- The department is bound by the provisions of the Electronic Transactions Act 1999 and so SMS/email signatures are permitted, providing certain criteria are met. We touched on this briefly in bulletin 3, point 5 https://synapsemedical.com.au/news/2020/03/18/covid-mbs-items-explainer-and-faqs-no-3-18-march-2020/ .
Take home messages
- Obtain whatever evidence of COVID items bulk billing consent you can and write it down
- Don’t agonise over it. Do your best, be transparent always, and keep good records.
- And remember the department has said you don’t need to retain DB4 vouchers anyway so…
More later this evening
Margaret and the Synapse team
COVID MBS items explainer and FAQs No. 15, 31 March 2020… Read more
- Privacy Policy
- Terms and Conditions
Commonwealth Consolidated Acts
Search austlii.
- All databases
- This database only
- This legisation only
- Titles only
- Advanced Search…
- Copyright & Usage
- Disclaimers
All Databases
Cases & legislation, journals & scholarship, communities, new zealand, specific year, health insurance act 1973 - sect 20a assignment of medicare benefit.
- Next Section
- Previous Section
- Table of Provisions
- Print (pretty)
- Print (eco-friendly)
No downloadable files available
- NoteUp references
Join the discussion
- Tweet this page
- Follow @AustLII on Twitter
- Recent tweets about AustLII
- Individuals myGov is a simple and secure way to access online government services.
- PRODA Log in to access HPOS, Business Hub, Aged Care Provider Portal and a range of other government online services.
- Centrelink Business Online
- Child Support Business Online
Bulk bill payments to health professionals
Information to help you with Medicare bulk billing.
on this page
Assigning the benefit, making additional charges, bulk billing and private billing together, claiming bulk bill payments, getting your bulk bill payment, lodging a bulk bill claim late, adjusting a bulk bill claim.
Bulk billing is when you bill Medicare directly for your patient’s medical or allied health service.
In a bulk billing arrangement both of the following apply:
- you accept the Medicare benefit as full payment for the service
- your patient assigns their right to a Medicare benefit to you, so we pay the benefit to you.
A patient assigns their right to a Medicare benefit to you by signing a completed assignment of benefit form.
Use the approved assignment of benefit form for manual claims. For online claiming you can print the assignment of benefit statement from your practice management software.
By signing the form, your patient assigns their right to a Medicare benefit to you.
A patient or other responsible person must not sign a blank or incomplete assignment of benefit form.
Assignment of benefit and signature requirements
You need your patient's agreement to bulk bill the items before we can pay you the Medicare benefit.
Read more about Assignment of benefit signature requirements and permissible exemptions .
If you bulk bill a patient, you can’t charge the patient an additional amount for that service.
This includes, but isn’t limited to:
- any consumables used, including bandages and dressings
- record keeping fees
- a booking fee to be paid before each service
- an annual administration or registration fee.
An exception applies only to general practitioners and other non-specialist health professionals for attendance items 3 to 96 and 5000 to 5267 (inclusive): when you give the patient a vaccine or vaccines from your own supply at your practice.
It only relates to vaccines not available free of charge through Commonwealth or state funding, or Pharmaceutical Benefits Scheme. The additional charge can only cover the supply of the vaccine.
If you provide a number of services on a single occasion, you can both:
- bulk bill some or all of those services
- privately bill any you haven't bulked billed.
There's an exception if the Multiple Operational Rule affects any of these services. In this case you can use only one claiming channel for all the services, either bulk bill or private bill.
This also applies to the diagnostic imaging multiple services rules (DIMSR).
If you bulk bill a service, both of these apply:
- you accept the patient's Medicare benefit as full payment for the service
- you can't charge an additional fee.
If you only bulk bill some of the services, you can charge an additional fee privately for the other services.
Choosing to bill this way means you can set the charge.
This includes the amount to compensate for the use of consumables or to cover other costs. You can only charge the additional fee if it relates to the service you're claiming.
You need to lodge a bulk bill claim within 2 years from the date of service. Read about bulk bill late lodgements for claims older than 2 years.
Electronic claims
You can submit bulk bill claims electronically through either:
- Medicare Online for health professionals
- Medicare Easyclaim
If you want to claim both in-hospital and out of hospital services, you'll need to submit them in separate claims.
If you need the patient’s consent on the assignment of benefit before submitting your claim electronically, use the HPOS bulk bill Webclaim form .
You can submit claims electronically if the health professional getting the payment is a short-term locum and doesn't have a provider number.
We no longer send cheques for bulk bill and Department of Veterans' Affairs (DVA) payments to health professionals.
You must give us your bank details to get your bulk bill and DVA claims paid through Electronic Funds Transfer (EFT).
If you practice at more than one location, you must submit bank details for each location.
Providing your details
Give us your bank details by registering for EFT payments using Medicare online claiming or Medicare Easyclaim .
To register for EFT payments, fill in and submit both these forms:
- Provider registration for Electronic Funds Transfer payments form
- Online Claiming Provider Agreement form .
You must lodge a Medicare claim with us within 2 years from the date of service. This is outlined in the Health Insurance Act 1973 section 20B(2)(b).
Read about bulk bill late lodgements .
You can call the Medicare provider enquiries line to delete a claim you lodge on that day.
You can change an item number or other details on a processed claim that’s under 2 years old.
The table below shows how to submit a request for an adjustment.
Your patient must sign any changes to their information. This is because you’re changing the original agreement you made with the patient to accept the patient’s assigned benefits.
You can’t request an adjustment unless a new assignment of benefit form has been signed by your patient or a third party .
Changing a paid or omitted bulk bill incentive or PEI item
We’ll accept requests to change a previously paid bulk bill claim if the date of service is within 2 years. This applies to both omitted items and item changes.
The table below shows how to submit changes to previously paid bulk bill incentive or patient episode initiation (PEI) items.
Bulk bill adjustment statements
When we process an adjustment for bulk billing, we’ll send you a bulk bill adjustment statement.
These statements now show all service lines for the patient, rather than just the service lines that had been adjusted.
The result line will show the difference between the original and revised service lines.
The following tables show the reason codes we use in adjustment statements. They include codes for:
- an underpayment
- an overpayment
- statistical bulk bill adjustment.
Underpayment of the previous benefit paid
Overpayment of the previous benefit paid, statistical bulk bill adjustment.
Contact the eBusiness service centre for more information.
The Health Insurance Act 1973, section 20B(2)(b), states that a Medicare claim must be lodged with us within 2 years from the date of service.
This information was printed 11 April 2024 from https://www.servicesaustralia.gov.au/bulk-bill-payments-to-health-professionals . It may not include all of the relevant information on this topic. Please consider any relevant site notices at https://www.servicesaustralia.gov.au/site-notices when using this material.
Printed link references
IMAGES
VIDEO
COMMENTS
Assignment of Medicare benefit. (1) Where a , the first-mentioned by whom, or on whose behalf, the is rendered (in this ) may enter into an agreement, in accordance with the. (a) the first-mentioned assigns his or her right to the payment of the. (b) the accepts the assignment in full payment of the incurred in respect of the by the first ...
What is the assignment of benefit rule? The requirement for a patient's signature is considered an important deterrent to fraud (eg claims for services that were not provided). The DoHAC is obligated to enforce these rules under section 20A of the Health Insurance Act 1973.
If your doctor, provider, or supplier doesn't accept assignment: You might have to pay the full amount at the time of service. They should submit a claim to Medicare for any Medicare-covered services they give you, and they can't charge you for submitting a claim. If they refuse to submit a Medicare claim, you can submit your own claim to ...
Here's how it works: Medicare will pay the provider 95% of the amount they would pay if the provider accepted assignment. The provider can charge the person receiving care more than the Medicare-approved amount, but only up to 15% more (some states limit this further). This extra amount, which the patient has to pay out-of-pocket, is known as ...
Medicare assignment is a fee schedule agreement between the federal government's Medicare program and a doctor or facility. When Medicare assignment is accepted, it means your doctor agrees to the payment terms of Medicare. Doctors that accept Medicare assignment fall under one of three designations: a participating doctor, a non ...
patient's Medicare benefit as full payment for a service. When a practitioner bulk bills a patient, the practitioner can receive the Medicare benefit for the service directly from Services Australia, using the online claiming facility. Section 20A of the Act provides for bulk billing. For an assignment of benefit in accordance with Section
"Medicare Agreement (Section 20A of the Health Insurance Act 1973) I offer to assign my right to benefits to the approved pathology practitioner who will render the requested pathology service(s) and any eligible pathologist determinable service(s) established as necessary by the practitioner. ... Assignment of benefits requires the patient to ...
Bulk billing (where Medicare does pay doctors directly) hinges on section 20A of the Act. What section 20A says is that a patient can assign their Medicare benefit to their treating doctor by signing the approved form, where the approved form is the form approved in writing by the minister. The approved form is called a DB4 form.
Section 20A of the Act provides for bulk billing. For an assignment of benefit in accordance with Section 20A, there must be an agreement under which the patient (or person responsible for the medical expenses such as a parent of a patient) assigns their right to a Medicare benefit to the practitioner who must accept it as 'full payment of ...
Medicare Assignment: (Section 20A of the Health Insurance Act 1973) I assign my right to benefits to the approved pathology practitioner who will render the requested pathology service(s) and any eligible pathologist determinable service(s). Patient Account Statement: Your doctor has requested tests, according to clinical need.
the Medicare benefit for the service directly from Services Australia, using the online claiming facility. Section 20A of the Act provides for bulk billing. For an assignment of benefit in accordance with Section 20A, there must be an agreement under which the patient (or person responsible for the medical expenses such as a parent of a
"20A Assignment of Medicare benefit (1) ... Section 20A and 20B remain in force. Further, these important machinery provisions of the Medicare scheme are unlikely to ever be changed because it would require a parliamentary process, which would be unlikely to succeed because it would be just too damaging to the scheme. ...
You must not write 'patient deceased' as a reason for not getting a signature on the assignment of benefit form. Email agreement. Follow the steps in the table below when a patient assigns their right to a Medicare benefit to you by email. For privacy reasons, don't include the Medicare card number and provider number in the email.
HEALTH INSURANCE ACT 1973 - SECT 20A Assignment of Medicare benefit HEALTH INSURANCE ACT 1973 - SECT 20A Assignment of Medicare benefit (1) Where a medicare benefit is payable to an eligible person in respect of a professional service rendered to the eligible person or to another eligible person, the first-mentioned eligible person and the person by whom, or on whose behalf, the professional ...
MEDICARE ASSIGNMENT (Section 20A of the Health Insurance Act 1973): I offer to assign my right to benefits to the Approved Pathology Practitioner : who will render the requested pathology service(s) and any eligible pathologist determinable service(s) established as necessary by the practitioner.
MEDICARE ASSIGNMENT (Section 20A of the Health Insurance Act 1973): I offer to assign my right to benefits to the approved pathology practitioner who will render the requested pathology service(s) and any eligible pathologist determinable service(s) established as necessary by the practitioner.
Use this form in conjunction with HPOS Medicare Bulk Bill Webclaims only. It cannot be submitted to us for manual processing. Download and complete the Assignment of benefit Medicare bulk bill Webclaim form. This form is interactive. It has 2 copies, one for the health professional and one for the patient. If you have a disability or impairment ...
MEDICARE ASSIGNMENT FORM (Section 20A of the Health Insurance Act 1973) I assign my right to benefits to the approved pathology practitioner who will render the requested pathology service(s) and any eligible pathologist determinable service(s) as necessary by the practitioner.
MEDICARE ASSIGNMENT (Section 20A of the Health Insurance Act 1973) I offer to assign my right to benefits to the approved pathology practitioner who will render the requested pathology service(s) and any eligible pathologist determinable service(s) established as necessary by the practitioner. In the alternate I authorise Australian Clinical ...
Getting your bulk bill payment. Lodging a bulk bill claim late. Adjusting a bulk bill claim. Bulk billing is when you bill Medicare directly for your patient's medical or allied health service. In a bulk billing arrangement both of the following apply: you accept the Medicare benefit as full payment for the service.
MEDICARE ASSIGNMENT (Section 20A of the Health Insurance Act 1973) X practitioner. Drug - Last Dose dorevitch.com.au Signature) ... Medicare Prostate-SpecificAntigen (PSA) billing criteria have been amended to align with NHMRC-endorsed guidelines2. These changes consider family history,
MEDICARE ASSIGNMENT (Section 20A of the Health Insurance Act 1973) I offer to assign my right to benefits to the approved pathology practitioner who will render the requested pathology service(s). And any eligible pathologist determinable service(s) established as necessary by the practioner.
MEDICARE ASSIGNMENT (Section 20A of the Health Insurance Act 1973) I offer to assign my right to benefits to the approved pathology practitioner who will render the requested . pathology service(s) and any eligible pathologist determinable service(s) established as necessary by the .