8 Lessons We Can Learn From the COVID-19 Pandemic
BY KATHY KATELLA May 14, 2021

Note: Information in this article was accurate at the time of original publication. Because information about COVID-19 changes rapidly, we encourage you to visit the websites of the Centers for Disease Control & Prevention (CDC), World Health Organization (WHO), and your state and local government for the latest information.
The COVID-19 pandemic changed life as we know it—and it may have changed us individually as well, from our morning routines to our life goals and priorities. Many say the world has changed forever. But this coming year, if the vaccines drive down infections and variants are kept at bay, life could return to some form of normal. At that point, what will we glean from the past year? Are there silver linings or lessons learned?
“Humanity's memory is short, and what is not ever-present fades quickly,” says Manisha Juthani, MD , a Yale Medicine infectious diseases specialist. The bubonic plague, for example, ravaged Europe in the Middle Ages—resurfacing again and again—but once it was under control, people started to forget about it, she says. “So, I would say one major lesson from a public health or infectious disease perspective is that it’s important to remember and recognize our history. This is a period we must remember.”
We asked our Yale Medicine experts to weigh in on what they think are lessons worth remembering, including those that might help us survive a future virus or nurture a resilience that could help with life in general.

Lesson 1: Masks are useful tools
What happened: The Centers for Disease Control and Prevention (CDC) relaxed its masking guidance for those who have been fully vaccinated. But when the pandemic began, it necessitated a global effort to ensure that everyone practiced behaviors to keep themselves healthy and safe—and keep others healthy as well. This included the widespread wearing of masks indoors and outside.
What we’ve learned: Not everyone practiced preventive measures such as mask wearing, maintaining a 6-foot distance, and washing hands frequently. But, Dr. Juthani says, “I do think many people have learned a whole lot about respiratory pathogens and viruses, and how they spread from one person to another, and that sort of old-school common sense—you know, if you don’t feel well—whether it’s COVID-19 or not—you don’t go to the party. You stay home.”
Masks are a case in point. They are a key COVID-19 prevention strategy because they provide a barrier that can keep respiratory droplets from spreading. Mask-wearing became more common across East Asia after the 2003 SARS outbreak in that part of the world. “There are many East Asian cultures where the practice is still that if you have a cold or a runny nose, you put on a mask,” Dr. Juthani says.
She hopes attitudes in the U.S. will shift in that direction after COVID-19. “I have heard from a number of people who are amazed that we've had no flu this year—and they know masks are one of the reasons,” she says. “They’ve told me, ‘When the winter comes around, if I'm going out to the grocery store, I may just put on a mask.’”
Lesson 2: Telehealth might become the new normal
What happened: Doctors and patients who have used telehealth (technology that allows them to conduct medical care remotely), found it can work well for certain appointments, ranging from cardiology check-ups to therapy for a mental health condition. Many patients who needed a medical test have also discovered it may be possible to substitute a home version.
What we’ve learned: While there are still problems for which you need to see a doctor in person, the pandemic introduced a new urgency to what had been a gradual switchover to platforms like Zoom for remote patient visits.
More doctors also encouraged patients to track their blood pressure at home , and to use at-home equipment for such purposes as diagnosing sleep apnea and even testing for colon cancer . Doctors also can fine-tune cochlear implants remotely .
“It happened very quickly,” says Sharon Stoll, DO, a neurologist. One group that has benefitted is patients who live far away, sometimes in other parts of the country—or even the world, she says. “I always like to see my patients at least twice a year. Now, we can see each other in person once a year, and if issues come up, we can schedule a telehealth visit in-between,” Dr. Stoll says. “This way I may hear about an issue before it becomes a problem, because my patients have easier access to me, and I have easier access to them.”
Meanwhile, insurers are becoming more likely to cover telehealth, Dr. Stoll adds. “That is a silver lining that will hopefully continue.”
Lesson 3: Vaccines are powerful tools
What happened: Given the recent positive results from vaccine trials, once again vaccines are proving to be powerful for preventing disease.
What we’ve learned: Vaccines really are worth getting, says Dr. Stoll, who had COVID-19 and experienced lingering symptoms, including chronic headaches . “I have lots of conversations—and sometimes arguments—with people about vaccines,” she says. Some don’t like the idea of side effects. “I had vaccine side effects and I’ve had COVID-19 side effects, and I say nothing compares to the actual illness. Unfortunately, I speak from experience.”
Dr. Juthani hopes the COVID-19 vaccine spotlight will motivate people to keep up with all of their vaccines, including childhood and adult vaccines for such diseases as measles , chicken pox, shingles , and other viruses. She says people have told her they got the flu vaccine this year after skipping it in previous years. (The CDC has reported distributing an exceptionally high number of doses this past season.)
But, she cautions that a vaccine is not a magic bullet—and points out that scientists can’t always produce one that works. “As advanced as science is, there have been multiple failed efforts to develop a vaccine against the HIV virus,” she says. “This time, we were lucky that we were able build on the strengths that we've learned from many other vaccine development strategies to develop multiple vaccines for COVID-19 .”
Lesson 4: Everyone is not treated equally, especially in a pandemic
What happened: COVID-19 magnified disparities that have long been an issue for a variety of people.
What we’ve learned: Racial and ethnic minority groups especially have had disproportionately higher rates of hospitalization for COVID-19 than non-Hispanic white people in every age group, and many other groups faced higher levels of risk or stress. These groups ranged from working mothers who also have primary responsibility for children, to people who have essential jobs, to those who live in rural areas where there is less access to health care.
“One thing that has been recognized is that when people were told to work from home, you needed to have a job that you could do in your house on a computer,” says Dr. Juthani. “Many people who were well off were able do that, but they still needed to have food, which requires grocery store workers and truck drivers. Nursing home residents still needed certified nursing assistants coming to work every day to care for them and to bathe them.”
As far as racial inequities, Dr. Juthani cites President Biden’s appointment of Yale Medicine’s Marcella Nunez-Smith, MD, MHS , as inaugural chair of a federal COVID-19 Health Equity Task Force. “Hopefully the new focus is a first step,” Dr. Juthani says.
Lesson 5: We need to take mental health seriously
What happened: There was a rise in reported mental health problems that have been described as “a second pandemic,” highlighting mental health as an issue that needs to be addressed.
What we’ve learned: Arman Fesharaki-Zadeh, MD, PhD , a behavioral neurologist and neuropsychiatrist, believes the number of mental health disorders that were on the rise before the pandemic is surging as people grapple with such matters as juggling work and childcare, job loss, isolation, and losing a loved one to COVID-19.
The CDC reports that the percentage of adults who reported symptoms of anxiety of depression in the past 7 days increased from 36.4 to 41.5 % from August 2020 to February 2021. Other reports show that having COVID-19 may contribute, too, with its lingering or long COVID symptoms, which can include “foggy mind,” anxiety , depression, and post-traumatic stress disorder .
“We’re seeing these problems in our clinical setting very, very often,” Dr. Fesharaki-Zadeh says. “By virtue of necessity, we can no longer ignore this. We're seeing these folks, and we have to take them seriously.”
Lesson 6: We have the capacity for resilience
What happened: While everyone’s situation is different (and some people have experienced tremendous difficulties), many have seen that it’s possible to be resilient in a crisis.
What we’ve learned: People have practiced self-care in a multitude of ways during the pandemic as they were forced to adjust to new work schedules, change their gym routines, and cut back on socializing. Many started seeking out new strategies to counter the stress.
“I absolutely believe in the concept of resilience, because we have this effective reservoir inherent in all of us—be it the product of evolution, or our ancestors going through catastrophes, including wars, famines, and plagues,” Dr. Fesharaki-Zadeh says. “I think inherently, we have the means to deal with crisis. The fact that you and I are speaking right now is the result of our ancestors surviving hardship. I think resilience is part of our psyche. It's part of our DNA, essentially.”
Dr. Fesharaki-Zadeh believes that even small changes are highly effective tools for creating resilience. The changes he suggests may sound like the same old advice: exercise more, eat healthy food, cut back on alcohol, start a meditation practice, keep up with friends and family. “But this is evidence-based advice—there has been research behind every one of these measures,” he says.
But we have to also be practical, he notes. “If you feel overwhelmed by doing too many things, you can set a modest goal with one new habit—it could be getting organized around your sleep. Once you’ve succeeded, move on to another one. Then you’re building momentum.”
Lesson 7: Community is essential—and technology is too
What happened: People who were part of a community during the pandemic realized the importance of human connection, and those who didn’t have that kind of support realized they need it.
What we’ve learned: Many of us have become aware of how much we need other people—many have managed to maintain their social connections, even if they had to use technology to keep in touch, Dr. Juthani says. “There's no doubt that it's not enough, but even that type of community has helped people.”
Even people who aren’t necessarily friends or family are important. Dr. Juthani recalled how she encouraged her mail carrier to sign up for the vaccine, soon learning that the woman’s mother and husband hadn’t gotten it either. “They are all vaccinated now,” Dr. Juthani says. “So, even by word of mouth, community is a way to make things happen.”
It’s important to note that some people are naturally introverted and may have enjoyed having more solitude when they were forced to stay at home—and they should feel comfortable with that, Dr. Fesharaki-Zadeh says. “I think one has to keep temperamental tendencies like this in mind.”
But loneliness has been found to suppress the immune system and be a precursor to some diseases, he adds. “Even for introverted folks, the smallest circle is preferable to no circle at all,” he says.
Lesson 8: Sometimes you need a dose of humility
What happened: Scientists and nonscientists alike learned that a virus can be more powerful than they are. This was evident in the way knowledge about the virus changed over time in the past year as scientific investigation of it evolved.
What we’ve learned: “As infectious disease doctors, we were resident experts at the beginning of the pandemic because we understand pathogens in general, and based on what we’ve seen in the past, we might say there are certain things that are likely to be true,” Dr. Juthani says. “But we’ve seen that we have to take these pathogens seriously. We know that COVID-19 is not the flu. All these strokes and clots, and the loss of smell and taste that have gone on for months are things that we could have never known or predicted. So, you have to have respect for the unknown and respect science, but also try to give scientists the benefit of the doubt,” she says.
“We have been doing the best we can with the knowledge we have, in the time that we have it,” Dr. Juthani says. “I think most of us have had to have the humility to sometimes say, ‘I don't know. We're learning as we go.’"
Information provided in Yale Medicine articles is for general informational purposes only. No content in the articles should ever be used as a substitute for medical advice from your doctor or other qualified clinician. Always seek the individual advice of your health care provider with any questions you have regarding a medical condition.
More news from Yale Medicine

Help inform the discussion
Presidential Speeches
September 9, 2021: remarks on fighting the covid-19 pandemic, about this speech.
September 09, 2021
As the Delta variant of the Covid-19 virus spreads and cases and deaths increase in the United States, President Joe Biden announces new efforts to fight the pandemic. He outlines six broad areas of action--implementing new vaccination requirements, protecting the vaccinated with booster shots, keeping children safe and schools open, increasing testing and masking, protecting our economic recovery, and improving care of those who do get Covid-19.
- Download Full Video
- Download Audio
THE PRESIDENT: Good evening, my fellow Americans. I want to talk to you about where we are in the battle against COVID-19, the progress we’ve made, and the work we have left to do.
And it starts with understanding this: Even as the Delta variant 19 [sic] has—COVID-19—has been hitting this country hard, we have the tools to combat the virus, if we can come together as a country and use those tools.
If we raise our vaccination rate, protect ourselves and others with masking and expanded testing, and identify people who are infected, we can and we will turn the tide on COVID-19.
It will take a lot of hard work, and it’s going to take some time. Many of us are frustrated with the nearly 80 million Americans who are still not vaccinated, even though the vaccine is safe, effective, and free.
You might be confused about what is true and what is false about COVID-19. So before I outline the new steps to fight COVID-19 that I’m going to be announcing tonight, let me give you some clear information about where we stand.
First, we have cons—we have made considerable progress
in battling COVID-19. When I became President, about 2 million Americans were fully vaccinated. Today, over 175 million Americans have that protection.
Before I took office, we hadn’t ordered enough vaccine for every American. Just weeks in office, we did. The week before I took office, on January 20th of this year, over 25,000 Americans died that week from COVID-19. Last week, that grim weekly toll was down 70 percent.
And in the three months before I took office, our economy was faltering, creating just 50,000 jobs a month. We’re now averaging 700,000 new jobs a month in the past three months.
This progress is real. But while America is in much better shape than it was seven months ago when I took office, I need to tell you a second fact.
We’re in a tough stretch, and it could last for a while. The highly contagious Delta variant that I began to warn America about back in July spread in late summer like it did in other countries before us.
While the vaccines provide strong protections for the vaccinated, we read about, we hear about, and we see the stories of hospitalized people, people on their death beds, among the unvaccinated over these past few weeks.
This is a pandemic of the unvaccinated. And it’s caused by the fact that despite America having an unprecedented and successful vaccination program, despite the fact that for almost five months free vaccines have been available in 80,000 different locations, we still have nearly 80 million Americans who have failed to get the shot.
And to make matters worse, there are elected officials actively working to undermine the fight against COVID-19. Instead of encouraging people to get vaccinated and mask up, they’re ordering mobile morgues for the unvaccinated dying from COVID in their communities. This is totally unacceptable.
Third, if you wonder how all this adds up, here’s the math: The vast majority of Americans are doing the right thing. Nearly three quarters of the eligible have gotten at least one shot, but one quarter has not gotten any. That’s nearly 80 million Americans not vaccinated. And in a country as large as ours, that’s 25 percent minority. That 25 percent can cause a lot of damage—and they are.
The unvaccinated overcrowd our hospitals, are overrunning the emergency rooms and intensive care units, leaving no room for someone with a heart attack, or pancreitis [pancreatitis], or cancer.
And fourth, I want to emphasize that the vaccines provide very strong protection from severe illness from COVID-19. I know there’s a lot of confusion and misinformation. But the world’s leading scientists confirm that if you are fully vaccinated, your risk of severe illness from COVID-19 is very low.
In fact, based on available data from the summer, only one of out of every 160,000 fully vaccinated Americans was hospitalized for COVID per day.
These are the facts.
So here’s where we stand: The path ahead, even with the Delta variant, is not nearly as bad as last winter. But what makes it incredibly more frustrating is that we have the tools to combat COVID-19, and a distinct minority of Americans –supported by a distinct minority of elected officials—are keeping us from turning the corner. These pandemic politics, as I refer to, are making people sick, causing unvaccinated people to die.
We cannot allow these actions to stand in the way of protecting the large majority of Americans who have done their part and want to get back to life as normal.
As your President, I’m announcing tonight a new plan to require more Americans to be vaccinated, to combat those blocking public health.
My plan also increases testing, protects our economy, and will make our kids safer in schools. It consists of six broad areas of action and many specific measures in each that—and each of those actions that you can read more about at WhiteHouse.gov. WhiteHouse.gov.
The measures—these are going to take time to have full impact. But if we implement them, I believe and the scientists indicate, that in the months ahead we can reduce the number of unvaccinated Americans, decrease hospitalizations and deaths, and allow our children to go to school safely and keep our economy strong by keeping businesses open.
First, we must increase vaccinations among the unvaccinated with new vaccination requirements. Of the nearly 80 million eligible Americans who have not gotten vaccinated, many said they were waiting for approval from the Food and Drug Administration—the FDA. Well, last month, the FDA granted that approval.
So, the time for waiting is over. This summer, we made progress through the combination of vaccine requirements and incentives, as well as the FDA approval. Four million more people got their first shot in August than they did in July.
But we need to do more. This is not about freedom or personal choice. It’s about protecting yourself and those around you—the people you work with, the people you care about, the people you love.
My job as President is to protect all Americans.
So, tonight, I’m announcing that the Department of Labor is developing an emergency rule to require all employers with 100 or more employees, that together employ over 80 million workers, to ensure their workforces are fully vaccinated or show a negative test at least once a week.
Some of the biggest companies are already requiring this: United Airlines, Disney, Tysons Food, and even Fox News.
The bottom line: We’re going to protect vaccinated workers from unvaccinated co-workers. We’re going to reduce the spread of COVID-19 by increasing the share of the workforce that is vaccinated in businesses all across America.
My plan will extend the vaccination requirements that I previously issued in the healthcare field. Already, I’ve announced, we’ll be requiring vaccinations that all nursing home workers who treat patients on Medicare and Medicaid, because I have that federal authority.
Tonight, I’m using that same authority to expand that to cover those who work in hospitals, home healthcare facilities, or other medical facilities–a total of 17 million healthcare workers.
If you’re seeking care at a health facility, you should be able to know that the people treating you are vaccinated. Simple. Straightforward. Period.
Next, I will sign an executive order that will now require all executive branch federal employees to be vaccinated—all. And I’ve signed another executive order that will require federal contractors to do the same.
If you want to work with the federal government and do business with us, get vaccinated. If you want to do business with the federal government, vaccinate your workforce.
And tonight, I’m removing one of the last remaining obstacles that make it difficult for you to get vaccinated.
The Department of Labor will require employers with 100 or more workers to give those workers paid time off to get vaccinated. No one should lose pay in order to get vaccinated or take a loved one to get vaccinated.
Today, in total, the vaccine requirements in my plan will affect about 100 million Americans—two thirds of all workers.
And for other sectors, I issue this appeal: To those of you running large entertainment venues—from sports arenas to concert venues to movie theaters—please require folks to get vaccinated or show a negative test as a condition of entry.
And to the nation’s family physicians, pediatricians, GPs—general practitioners—you’re the most trusted medical voice to your patients. You may be the one person who can get someone to change their mind about being vaccinated.
Tonight, I’m asking each of you to reach out to your unvaccinated patients over the next two weeks and make a personal appeal to them to get the shot. America needs your personal involvement in this critical effort.
And my message to unvaccinated Americans is this: What more is there to wait for? What more do you need to see? We’ve made vaccinations free, safe, and convenient.
The vaccine has FDA approval. Over 200 million Americans have gotten at least one shot.
We’ve been patient, but our patience is wearing thin. And your refusal has cost all of us. So, please, do the right thing. But just don’t take it from me; listen to the voices of unvaccinated Americans who are lying in hospital beds, taking their final breaths, saying, “If only I had gotten vaccinated.” “If only.”
It’s a tragedy. Please don’t let it become yours.
The second piece of my plan is continuing to protect the vaccinated.
For the vast majority of you who have gotten vaccinated, I understand your anger at those who haven’t gotten vaccinated. I understand the anxiety about getting a “breakthrough” case.
But as the science makes clear, if you’re fully vaccinated, you’re highly protected from severe illness, even if you get COVID-19.
In fact, recent data indicates there is only one confirmed positive case per 5,000 fully vaccinated Americans per day.
You’re as safe as possible, and we’re doing everything we can to keep it that way—keep it that way, keep you safe.
That’s where boosters come in—the shots that give you even more protection than after your second shot.
Now, I know there’s been some confusion about boosters. So, let me be clear: Last month, our top government doctors announced an initial plan for booster shots for vaccinated Americans. They believe that a booster is likely to provide the highest level of protection yet.
Of course, the decision of which booster shots to give, when to start them, and who will give them, will be left completely to the scientists at the FDA and the Centers for Disease Control.
But while we wait, we’ve done our part. We’ve bought enough boosters—enough booster shots—and the distribution system is ready to administer them.
As soon as they are authorized, those eligible will be able to get a booster right away in tens of thousands of site across the—sites across the country for most Americans, at your nearby drug store, and for free.
The third piece of my plan is keeping—and maybe the most important—is keeping our children safe and our schools open. For any parent, it doesn’t matter how low the risk of any illness or accident is when it comes to your child or grandchild. Trust me, I know.
So, let me speak to you directly. Let me speak to you directly to help ease some of your worries.
It comes down to two separate categories: children ages 12 and older who are eligible for a vaccine now, and children ages 11 and under who are not are yet eligible.
The safest thing for your child 12 and older is to get them vaccinated. They get vaccinated for a lot of things. That’s it. Get them vaccinated.
As with adults, almost all the serious COVID-19 cases we’re seeing among adolescents are in unvaccinated 12- to 17-year-olds—an age group that lags behind in vaccination rates.
So, parents, please get your teenager vaccinated.
What about children under the age of 12 who can’t get vaccinated yet? Well, the best way for a parent to protect their child under the age of 12 starts at home. Every parent, every teen sibling, every caregiver around them should be vaccinated.
Children have four times higher chance of getting hospitalized if they live in a state with low vaccination rates rather than the states with high vaccination rates.
Now, if you’re a parent of a young child, you’re wondering when will it be—when will it be—the vaccine available for them. I strongly support an independent scientific review for vaccine uses for children under 12. We can’t take shortcuts with that scientific work.
But I’ve made it clear I will do everything within my power to support the FDA with any resource it needs to continue to do this as safely and as quickly as possible, and our nation’s top doctors are committed to keeping the public at large updated on the process so parents can plan.
Now to the schools. We know that if schools follow the science and implement the safety measures—like testing, masking, adequate ventilation systems that we provided the money for, social distancing, and vaccinations—then children can be safe from COVID-19 in schools.
Today, about 90 percent of school staff and teachers are vaccinated. We should get that to 100 percent. My administration has already acquired teachers at the schools run by the Defense Department—because I have the authority as President in the federal system—the Defense Department and the Interior Department—to get vaccinated. That’s authority I possess.
Tonight, I’m announcing that we’ll require all of nearly 300,000 educators in the federal paid program, Head Start program, must be vaccinated as well to protect your youngest—our youngest—most precious Americans and give parents the comfort.
And tonight, I’m calling on all governors to require vaccination for all teachers and staff. Some already have done so, but we need more to step up.
Vaccination requirements in schools are nothing new. They work. They’re overwhelmingly supported by educators and their unions. And to all school officials trying to do the right thing by our children: I’ll always be on your side.
Let me be blunt. My plan also takes on elected officials and states that are undermining you and these lifesaving actions. Right now, local school officials are trying to keep children safe in a pandemic while their governor picks a fight with them and even threatens their salaries or their jobs. Talk about bullying in schools. If they’ll not help—if these governors won’t help us beat the pandemic, I’ll use my power as President to get them out of the way.
The Department of Education has already begun to take legal action against states undermining protection that local school officials have ordered. Any teacher or school official whose pay is withheld for doing the right thing, we will have that pay restored by the federal government 100 percent. I promise you I will have your back.
The fourth piece of my plan is increasing testing and masking. From the start, America has failed to do enough COVID-19 testing. In order to better detect and control the Delta variant, I’m taking steps tonight to make testing more available, more affordable, and more convenient. I’ll use the Defense Production Act to increase production of rapid tests, including those that you can use at home.
While that production is ramping up, my administration has worked with top retailers, like Walmart, Amazon, and Kroger’s, and tonight we’re announcing that, no later than next week, each of these outlets will start to sell at-home rapid test kits at cost for the next three months. This is an immediate price reduction for at-home test kits for up to 35 percent reduction.
We’ll also expand—expand free testing at 10,000 pharmacies around the country. And we’ll commit—we’re committing $2 billion to purchase nearly 300 million rapid tests for distribution to community health centers, food banks, schools, so that every American, no matter their income, can access free and convenient tests. This is important to everyone, particularly for a parent or a child—with a child not old enough to be vaccinated. You’ll be able to test them at home and test those around them.
In addition to testing, we know masking helps stop the spread of COVID-19. That’s why when I came into office, I required masks for all federal buildings and on federal lands, on airlines, and other modes of transportation.
Today—tonight, I’m announcing that the Transportation Safety Administration—the TSA—will double the fines on travelers that refuse to mask. If you break the rules, be prepared to pay.
And, by the way, show some respect. The anger you see on television toward flight attendants and others doing their job is wrong; it’s ugly.
The fifth piece of my plan is protecting our economic recovery. Because of our vaccination program and the American Rescue Plan, which we passed early in my administration, we’ve had record job creation for a new administration, economic growth unmatched in 40 years. We cannot let unvaccinated do this progress—undo it, turn it back.
So tonight, I’m announcing additional steps to strengthen our economic recovery. We’ll be expanding COVID-19 Economic Injury Disaster Loan programs. That’s a program that’s going to allow small businesses to borrow up to $2 million from the current $500,000 to keep going if COVID-19 impacts on their sales.
These low-interest, long-term loans require no repayment for two years and be can used to hire and retain workers, purchase inventory, or even pay down higher cost debt racked up since the pandemic began. I’ll also be taking additional steps to help small businesses stay afloat during the pandemic.
Sixth, we’re going to continue to improve the care of those who do get COVID-19. In early July, I announced the deployment of surge response teams. These are teams comprised of experts from the Department of Health and Human Services, the CDC, the Defense Department, and the Federal Emergency Management Agency—FEMA—to areas in the country that need help to stem the spread of COVID-19.
Since then, the federal government has deployed nearly 1,000 staff, including doctors, nurses, paramedics, into 18 states. Today, I’m announcing that the Defense Department will double the number of military health teams that they’ll deploy to help their fellow Americans in hospitals around the country.
Additionally, we’re increasing the availability of new medicines recommended by real doctors, not conspir-—conspiracy theorists. The monoclonal antibody treatments have been shown to reduce the risk of hospitalization by up to 70 percent for unvaccinated people at risk of developing sefe-—severe disease.
We’ve already distributed 1.4 million courses of these treatments to save lives and reduce the strain on hospitals. Tonight, I’m announcing we will increase the average pace of shipment across the country of free monoclonal antibody treatments by another 50 percent.
Before I close, let me say this: Communities of color are disproportionately impacted by this virus. And as we continue to battle COVID-19, we will ensure that equity continues to be at the center of our response. We’ll ensure that everyone is reached. My first responsibility as President is to protect the American people and make sure we have enough vaccine for every American, including enough boosters for every American who’s approved to get one.
We also know this virus transcends borders. That’s why, even as we execute this plan at home, we need to continue fighting the virus overseas, continue to be the arsenal of vaccines.
We’re proud to have donated nearly 140 million vaccines over 90 countries, more than all other countries combined, including Europe, China, and Russia combined. That’s American leadership on a global stage, and that’s just the beginning.
We’ve also now started to ship another 500 million COVID vaccines—Pfizer vaccines—purchased to donate to 100 lower-income countries in need of vaccines. And I’ll be announcing additional steps to help the rest of the world later this month.
As I recently released the key parts of my pandemic preparedness plan so that America isn’t caught flat-footed when a new pandemic comes again—as it will—next month, I’m also going to release the plan in greater detail.
So let me close with this: We have so-—we’ve made so much progress during the past seven months of this pandemic. The recent increases in vaccinations in August already are having an impact in some states where case counts are dropping in recent days. Even so, we remain at a critical moment, a critical time. We have the tools. Now we just have to finish the job with truth, with science, with confidence, and together as one nation.
Look, we’re the United States of America. There’s nothing—not a single thing—we’re unable to do if we do it together. So let’s stay together.
God bless you all and all those who continue to serve on the frontlines of this pandemic. And may God protect our troops.
Get vaccinated.
More Joe Biden speeches
- Armenia response
- Gaza response
- High contrast
- Press centre
Search UNICEF
Lessons we will learn from this pandemic, unicef young reporters shed light on the lessons they have learned during the covid-19 pandemic.

There is no rainbow without rain
Eva Hadzipetrova (15), UNICEF Young Reporter
I’ve been thinking a lot - what is it that will come out of all this? Equality! This situation has shown us that we are all the same regardless of our religion, culture, customs, whether we are poor or rich. The virus simply does not choose. It connected us in a way, it showed us that we should all stick together. During this chaos, while many of us in a panic, it showed us the weight of humanity. It reminded us who we are. Maybe the world will finally change.
We humans are fragile by ourselves. Our strength lies in being part of a community.
We do not live without relationships and we should never forget that. We have a very caring and shared connection between us and it’s amazing to see how we stick together at times. Sharing is caring. Sometimes we need to remember how important kindness is. We need to remember that we have been given a gift called life and that we should appreciate it.
Everything can end tomorrow. Focus on what is important to us. When all this is over, Earth will continue to spin, and life will flow again. The question is whether by then we will have learned our lesson. Let us be mindful of our Earth and it will be kind to us. There is no rainbow without rain. Remember that.

There is good in every evil
Maria Mitrikeska (15), UNICEF Young Reporter
There is an old saying ‘there is good in every evil’ that I will now use as a tiny consolation in this difficult, unexpected time. As a young teenager, believe me it is hard dealing with this situation, and to everyone who is reading this and feeling helpless, I just want to tell you that you are not alone, and it will be better!
I am aware of everything that has been taken away from us due to this situation, of all the unrealized plans, be it birthdays, travels, weddings ... and sadly, we cannot do anything about it. But we are not powerless! On the contrary, it is all of us together that can make the world a better place. If each of us respects the measures imposed by authorities, the situation will get better and it will pass much faster than expected.
I can single out isolation - staying at home – as one of the most important measures. I know it sounds difficult and believe me, at first this sounded impossible to me, just unfeasible. I found it hard and boring, I wasn’t used to sitting in the same closed place for so long. But over time, I started to find hobbies. I tried things I had never tried before. I spent a lot more time with my parents than before, and even though I didn’t go out, I exercised at home. I found I had the time to watch the TV series and read books I never had the time for! Also, I have to admit that for me, online learning is much easier, more flexible and stress-free.
One of the most important things I’ve learned while we’re in isolation is to take care of myself and to devote more time to myself.
Taking care of yourself is something so underestimated nowadays. Whether due to a lack of time or due to too much stress in everyday life or for a whatever reason, people don’t devote enough time to themselves. While in isolation, I’ve had a lot of time to think and realize that actually taking care of myself is one of the things that makes me happy. I mean little things that I believe are available to everyone. These little things are actually the ones that help me find myself.
Let’s go back to the sentence “There is good in every evil”. A simple short sentence, but still so powerful! This is just one perspective of a young girl who is going through the same thing as many others. So don’t forget, you’re never alone!

A pandemic that taught me to love
Branislav Maksimovski (15), UNICEF Young Reporter
It’ll take just a little patience and support for us to master this crisis, but together can we do it. We only need to respect the recommendations and measures issued by the state, to protect ourselves, the people closest to us, and others who live in our community. We all know that it is not easy to stay at home but taking a break to stop and reflect has its own virtues.
If someone asks me how I’m dealing with the pandemic and how it influences me I would say:
I know that is not easy for us, I know it’s not easy for those lying in the hospitals, I know it’s not easy for those who lost someone. Life takes us in different directions. That’s why it’s important to live the moment, without thinking of the past or the future. I sit at home, do my school assignments, go out on the balcony, have a tee or coffee, listen to good music. I can’t count all the activities I do to stay positive. It matters to me that my brother, my parents and grandparents are safe and for them I do my best. I write essays, I paint, I read. This situation has taught me many things.
It taught me to love, to listen, to care, to respect and to help.
Help - that’s the word I’m looking for. What does it mean “to help someone”? Help someone to teach them something. Help someone by having a conversation with them. We should use this word in our vocabulary more often, so we can see a smile on people’s faces more often. This situation taught me to love. Not only to love a person, but also to love the little things in life.

Life is a lesson, we learn and continue to learn every day
Andrijana Kamcheva (25), UNICEF Young Reporter
Humans are very complex beings; they spend their whole life learning. But why wait for something bad to happen so that we learn how to appreciate the good? Why can’t we appreciate the little things that actually make us happy?
I never had a chance to think about the things that have happened to me. I wasn’t appreciating many things and I have given importance to so many things, which weren’t important at all. I didn’t know that the rain makes me happy or that the coffee I have on the balcony is tastier than the coffee in a coffee shop. I realize that reading books makes me happy. Playing cards and monopoly at home wasn’t that bad at all and working out at home is better that at a gym. I realized that I’m a philanthropist and have a great sense of empathy, which makes me very happy.
We learn how to live every day. We choose the path we will take.
Just think about everything you dream of? It is good that we dream and work towards achieving a goal. Don’t be afraid to work miracles on yourself, don’t be afraid to live as you deserve. Its normal to come across obstacles, that’s how we learn when we overcome challenges.
Life is a lesson; we learn every day and we will continue learning every day. Everything doesn’t have to be perfect in life for us to be happy and to appreciate ourselves and everything around us. We just have to be greatful. Remember that the best life lesson is learned during hard times and when we make mistakes.
Enjoy your life and appreciate what you have. Just think about the fact that there are people in the world with less. Be happy and positive for everything around you and you will become a stonger person.
Blogs written by UNICEF Young Reporters are part of a UNICEF volunteer initiative to give young people the space to share their own views on topics important to them. The work of the Young Reporters during COVID-19 pandemic is partly funded by USAID.
Related topics
More to explore, a key to mental wellbeing: knowing yourself and your feeling.
How UNICEF’s chatbot equips Ukrainian and Polish youth with knowledge, which helps them understand, express and manage their feelings
UNICEF and the US Embassy in the Czech Republic announce new initiative to support young refugees with employment that empowers
New online platform offers networking and learning
u-platform.by is the only youth platform in Belarus that brings together training, volunteering, fighting online bullying and more
Forward to dream
In Uzbekistan UNICEF Skills4Girls programme equips women and girls with much-needed digital skills
Persuasive Essay Guide
Persuasive Essay About Covid19
How to Write a Persuasive Essay About Covid19 | Examples & Tips
11 min read

People also read
A Comprehensive Guide to Writing an Effective Persuasive Essay
200+ Persuasive Essay Topics to Help You Out
Learn How to Create a Persuasive Essay Outline
30+ Free Persuasive Essay Examples To Get You Started
Read Excellent Examples of Persuasive Essay About Gun Control
Crafting a Convincing Persuasive Essay About Abortion
Learn to Write Persuasive Essay About Business With Examples and Tips
Check Out 12 Persuasive Essay About Online Education Examples
Persuasive Essay About Smoking - Making a Powerful Argument with Examples
Are you looking to write a persuasive essay about the Covid-19 pandemic?
Writing a compelling and informative essay about this global crisis can be challenging. It requires researching the latest information, understanding the facts, and presenting your argument persuasively.
But don’t worry! with some guidance from experts, you’ll be able to write an effective and persuasive essay about Covid-19.
In this blog post, we’ll outline the basics of writing a persuasive essay . We’ll provide clear examples, helpful tips, and essential information for crafting your own persuasive piece on Covid-19.
Read on to get started on your essay.
- 1. Steps to Write a Persuasive Essay About Covid-19
- 2. Examples of Persuasive Essay About Covid19
- 3. Examples of Persuasive Essay About Covid-19 Vaccine
- 4. Examples of Persuasive Essay About Covid-19 Integration
- 5. Examples of Argumentative Essay About Covid 19
- 6. Examples of Persuasive Speeches About Covid-19
- 7. Tips to Write a Persuasive Essay About Covid-19
- 8. Common Topics for a Persuasive Essay on COVID-19
Steps to Write a Persuasive Essay About Covid-19
Here are the steps to help you write a persuasive essay on this topic, along with an example essay:
Step 1: Choose a Specific Thesis Statement
Your thesis statement should clearly state your position on a specific aspect of COVID-19. It should be debatable and clear. For example:
Step 2: Research and Gather Information
Collect reliable and up-to-date information from reputable sources to support your thesis statement. This may include statistics, expert opinions, and scientific studies. For instance:
- COVID-19 vaccination effectiveness data
- Information on vaccine mandates in different countries
- Expert statements from health organizations like the WHO or CDC
Step 3: Outline Your Essay
Create a clear and organized outline to structure your essay. A persuasive essay typically follows this structure:
- Introduction
- Background Information
- Body Paragraphs (with supporting evidence)
- Counterarguments (addressing opposing views)
Step 4: Write the Introduction
In the introduction, grab your reader's attention and present your thesis statement. For example:
Step 5: Provide Background Information
Offer context and background information to help your readers understand the issue better. For instance:
Step 6: Develop Body Paragraphs
Each body paragraph should present a single point or piece of evidence that supports your thesis statement. Use clear topic sentences, evidence, and analysis. Here's an example:
Step 7: Address Counterarguments
Acknowledge opposing viewpoints and refute them with strong counterarguments. This demonstrates that you've considered different perspectives. For example:
Step 8: Write the Conclusion
Summarize your main points and restate your thesis statement in the conclusion. End with a strong call to action or thought-provoking statement. For instance:
Step 9: Revise and Proofread
Edit your essay for clarity, coherence, grammar, and spelling errors. Ensure that your argument flows logically.
Step 10: Cite Your Sources
Include proper citations and a bibliography page to give credit to your sources.
Remember to adjust your approach and arguments based on your target audience and the specific angle you want to take in your persuasive essay about COVID-19.

Paper Due? Why Suffer? That's our Job!
Examples of Persuasive Essay About Covid19
When writing a persuasive essay about the Covid-19 pandemic, it’s important to consider how you want to present your argument. To help you get started, here are some example essays for you to read:
Check out some more PDF examples below:
Persuasive Essay About Covid-19 Pandemic
Sample Of Persuasive Essay About Covid-19
Persuasive Essay About Covid-19 In The Philippines - Example
If you're in search of a compelling persuasive essay on business, don't miss out on our “ persuasive essay about business ” blog!
Examples of Persuasive Essay About Covid-19 Vaccine
Covid19 vaccines are one of the ways to prevent the spread of Covid-19, but they have been a source of controversy. Different sides argue about the benefits or dangers of the new vaccines. Whatever your point of view is, writing a persuasive essay about it is a good way of organizing your thoughts and persuading others.
A persuasive essay about the Covid-19 vaccine could consider the benefits of getting vaccinated as well as the potential side effects.
Below are some examples of persuasive essays on getting vaccinated for Covid-19.
Covid19 Vaccine Persuasive Essay
Persuasive Essay on Covid Vaccines
Interested in thought-provoking discussions on abortion? Read our persuasive essay about abortion blog to eplore arguments!
Examples of Persuasive Essay About Covid-19 Integration
Covid19 has drastically changed the way people interact in schools, markets, and workplaces. In short, it has affected all aspects of life. However, people have started to learn to live with Covid19.
Writing a persuasive essay about it shouldn't be stressful. Read the sample essay below to get idea for your own essay about Covid19 integration.
Persuasive Essay About Working From Home During Covid19
Searching for the topic of Online Education? Our persuasive essay about online education is a must-read.
Examples of Argumentative Essay About Covid 19
Covid-19 has been an ever-evolving issue, with new developments and discoveries being made on a daily basis.
Writing an argumentative essay about such an issue is both interesting and challenging. It allows you to evaluate different aspects of the pandemic, as well as consider potential solutions.
Here are some examples of argumentative essays on Covid19.
Argumentative Essay About Covid19 Sample
Argumentative Essay About Covid19 With Introduction Body and Conclusion
Looking for a persuasive take on the topic of smoking? You'll find it all related arguments in out Persuasive Essay About Smoking blog!
Examples of Persuasive Speeches About Covid-19
Do you need to prepare a speech about Covid19 and need examples? We have them for you!
Persuasive speeches about Covid-19 can provide the audience with valuable insights on how to best handle the pandemic. They can be used to advocate for specific changes in policies or simply raise awareness about the virus.
Check out some examples of persuasive speeches on Covid-19:
Persuasive Speech About Covid-19 Example
Persuasive Speech About Vaccine For Covid-19
You can also read persuasive essay examples on other topics to master your persuasive techniques!
Tips to Write a Persuasive Essay About Covid-19
Writing a persuasive essay about COVID-19 requires a thoughtful approach to present your arguments effectively.
Here are some tips to help you craft a compelling persuasive essay on this topic:
Choose a Specific Angle
Start by narrowing down your focus. COVID-19 is a broad topic, so selecting a specific aspect or issue related to it will make your essay more persuasive and manageable. For example, you could focus on vaccination, public health measures, the economic impact, or misinformation.
Provide Credible Sources
Support your arguments with credible sources such as scientific studies, government reports, and reputable news outlets. Reliable sources enhance the credibility of your essay.
Use Persuasive Language
Employ persuasive techniques, such as ethos (establishing credibility), pathos (appealing to emotions), and logos (using logic and evidence). Use vivid examples and anecdotes to make your points relatable.
Organize Your Essay
Structure your essay involves creating a persuasive essay outline and establishing a logical flow from one point to the next. Each paragraph should focus on a single point, and transitions between paragraphs should be smooth and logical.
Emphasize Benefits
Highlight the benefits of your proposed actions or viewpoints. Explain how your suggestions can improve public health, safety, or well-being. Make it clear why your audience should support your position.
Use Visuals -H3
Incorporate graphs, charts, and statistics when applicable. Visual aids can reinforce your arguments and make complex data more accessible to your readers.
Call to Action
End your essay with a strong call to action. Encourage your readers to take a specific step or consider your viewpoint. Make it clear what you want them to do or think after reading your essay.
Revise and Edit
Proofread your essay for grammar, spelling, and clarity. Make sure your arguments are well-structured and that your writing flows smoothly.
Seek Feedback
Have someone else read your essay to get feedback. They may offer valuable insights and help you identify areas where your persuasive techniques can be improved.
Tough Essay Due? Hire Tough Writers!
Common Topics for a Persuasive Essay on COVID-19
Here are some persuasive essay topics on COVID-19:
- The Importance of Vaccination Mandates for COVID-19 Control
- Balancing Public Health and Personal Freedom During a Pandemic
- The Economic Impact of Lockdowns vs. Public Health Benefits
- The Role of Misinformation in Fueling Vaccine Hesitancy
- Remote Learning vs. In-Person Education: What's Best for Students?
- The Ethics of Vaccine Distribution: Prioritizing Vulnerable Populations
- The Mental Health Crisis Amidst the COVID-19 Pandemic
- The Long-Term Effects of COVID-19 on Healthcare Systems
- Global Cooperation vs. Vaccine Nationalism in Fighting the Pandemic
- The Future of Telemedicine: Expanding Healthcare Access Post-COVID-19
In search of more inspiring topics for your next persuasive essay? Our persuasive essay topics blog has plenty of ideas!
To sum it up,
You have read good sample essays and got some helpful tips. You now have the tools you needed to write a persuasive essay about Covid-19. So don't let the doubts stop you, start writing!
If you need professional writing help, don't worry! We've got that for you as well.
MyPerfectWords.com is a professional persuasive essay writing service that can help you craft an excellent persuasive essay on Covid-19. Our experienced essay writer will create a well-structured, insightful paper in no time!
So don't hesitate and place your ' write my essay online ' request today!
Frequently Asked Questions
Are there any ethical considerations when writing a persuasive essay about covid-19.
Yes, there are ethical considerations when writing a persuasive essay about COVID-19. It's essential to ensure the information is accurate, not contribute to misinformation, and be sensitive to the pandemic's impact on individuals and communities. Additionally, respecting diverse viewpoints and emphasizing public health benefits can promote ethical communication.
What impact does COVID-19 have on society?
The impact of COVID-19 on society is far-reaching. It has led to job and economic losses, an increase in stress and mental health disorders, and changes in education systems. It has also had a negative effect on social interactions, as people have been asked to limit their contact with others.

Write Essay Within 60 Seconds!

Caleb S. has been providing writing services for over five years and has a Masters degree from Oxford University. He is an expert in his craft and takes great pride in helping students achieve their academic goals. Caleb is a dedicated professional who always puts his clients first.

Paper Due? Why Suffer? That’s our Job!
Keep reading

- Skip to main content
- Skip to FDA Search
- Skip to in this section menu
- Skip to footer links

The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
U.S. Food and Drug Administration
- Search
- Menu
- News & Events
- Speeches by FDA Officials
- Remarks by Commissioner Stephen Hahn, M.D. — The COVID-19 Pandemic — Finding Solutions, Applying Lessons Learned - 06/01/2020
Speech | Virtual
Event Title Remarks by Commissioner Stephen Hahn, M.D. — The COVID-19 Pandemic — Finding Solutions, Applying Lessons Learned June 1, 2020
The COVID-19 Pandemic — Finding Solutions, Applying Lessons Learned
(Remarks as prepared for delivery. The text and video of this speech are slightly, though not substantively different from the version presented by Dr. Hahn on June 1 to the Alliance for a Stronger FDA, via audio broadcast only. Because of evolving scheduling challenges, it was not clear whether Dr. Hahn would be able to present the speech live and so it was recorded by video earlier. Ultimately, he did give the speech live to the Alliance, but only via an audio link. Given the minimal changes in the live version, we are posting the video version and the accompanying text.)
One of the most frustrating challenges each of us can face is the inability to control the events that affect our lives. Often, we are thrust into situations not of our own making. It’s no surprise that one of the most familiar adages concerns the best laid plans of mice and men going awry.
And yet, to borrow another often-used saying, necessity is the mother of invention. History teaches us that crises often lead to accelerated change and innovations and new discoveries.
This dynamic has been on my mind a great deal recently. It wasn’t too long ago – last December, to be exact -- that I had the distinction of being confirmed as the 24th Commissioner of the Food and Drug Administration.
This is the greatest honor of my life. I have long cherished the critical role the FDA plays in protecting and promoting the public health, and I’ve relied on the Agency’s expertise throughout my professional life.
So, I eagerly embraced my new responsibilities and the chance to make a real difference in public health. I was especially conscious that we live in a time of extraordinary scientific achievement, especially in oncology, with unprecedented opportunities to help make the lives of American patients and consumers healthier and safer.
I quickly immersed myself in the Agency’s broad and complex responsibilities, seizing every opportunity to learn about the FDA, both those areas with which I’d previously had minimum involvement, such as food policy, and those with which I had more familiarity, like cancer treatments and innovative clinical trial design.
I began to work with, and learn from, the agency’s extraordinary leadership team. I learned very quickly that the principles that have guided me throughout my life, such as my commitment to relying only on the best medical science and most rigorous data in support of advancing innovation and discovery, and my fundamental belief in promoting integrity and transparency in the scientific process, are the same principles that guide the FDA in both science and regulation.
So, I was in the midst of transitioning from being Chief Medical Executive at MD Anderson Cancer Center to being Commissioner of FDA when our entire world was turned upside down with the appearance of the novel COVID-19 coronavirus.
I certainly did not anticipate a public health emergency of this magnitude when I joined the agency. And I could not have imagined how significantly my new role would change and be shaped by this pandemic. I definitely could not have known that discussions about personal protective equipment (or PPE) or face masks or nasal swabs would be central to my work as Commissioner.
One thing was apparent: I would need to manage this evolving situation even as I was still learning about FDA.
From the very start I knew that even in a crisis situation – or perhaps especially because we are in a crisis situation – it is imperative that we maintain FDA’s high standards for evaluating products and making sure that the benefits outweigh potential harms.
To maintain our standard, I pledged to myself and emphasized to my new colleagues at FDA that our decisions would always be rooted in science. Having spent my entire career as a physician and scientist caring for patients with cancer, I’ve always valued highly a commitment to good data and sound science. I feel comfortable working with the scientists at FDA because I know they not only share that value, that commitment, but that they will tolerate nothing less. So, it was critical to me, as the pandemic escalated that this be reinforced as the guidepost for all of our decisions.
It may have been trial by fire, but I have the good fortune to work with an enormous number of talented individuals and teams who are helping guide us through this crisis. Every day they show extraordinary expertise, commitment, and resilience.
I also was able to call on many from outside the agency, including former FDA leaders as well as colleagues from the medical community.
What struck me was the uniformity of their advice. Those who formerly worked at FDA urged me to rely upon the FDA staff, many of whom have the experience to help manage a pandemic. My friends from outside the agency urged that we move quickly to make decisions, set direction and to be transparent about what we are doing. I have tried to follow all of this excellent advice.
Protecting the Food Supply
Since this crisis and the actions of the FDA have evolved so rapidly, let me summarize what we have done. I am confident that the FDA has measured up to this unprecedented challenge.
I want to start with the first word in the FDA’s name – food. Most of us take food safety for granted. But it takes a lot of hard work to maintain a safe food supply. This was true even before the COVID-19 pandemic but is especially challenging during an ongoing international crisis.
During the pandemic, through the collaboration of the FDA, the food industry and our federal and state partners, we have been able to maintain the safety of the nation’s food supply. Our Coordinated Outbreak Response and Evaluation team remained on the job, monitoring for signs of foodborne illness outbreaks and prepared to take action when needed.
And along with our federal partners, including CDC and USDA, we also have provided best practices for food workers, industry, and consumers on how to stay safe and keep food safe.
Diagnosing and Developing Treatments
On the medical side, we immediately committed to facilitating efforts to develop diagnostic tests, treatments and vaccines for the disease. We have helped facilitate increases in our national testing capacity, have helped ensure continued access to necessary medical products, and have sought to prevent the sale of fraudulent products.
If there’s one thing that’s been reaffirmed during this crisis, it’s the essential role of medical devices, including diagnostics, to countering this pandemic.
From the earliest days of our response, we worked to ensure that we had the essential medical devices, including personal protective equipment, to help treat those who are ill and to ensure that health care workers and others on the front line are properly protected.
To be sure, there were bumps along the road, but today we have an adequate supply of the devices that have been in unprecedented high demand such as PPE, ventilators, and others.
We’ve reviewed and issued emergency use authorizations for medical devices for COVID-19 at an incredibly fast pace.
And we’ve worked closely with many companies that don’t regularly make medical products but wanted to pitch in by making hand sanitizer, ventilators, or PPE.
There was a special focus on the development and availability of accurate and reliable COVID-19 tests. We need to know who has the disease and who has had it. This is essential if we are to understand this virus and return to a more normal lifestyle.
Since January, we’ve worked with hundreds of test developers, many of whom have submitted emergency use authorization requests to FDA for tests that detect the virus or antibodies to the virus.
As you have seen reported, early in the crisis we provided regulatory flexibility for developers with validated tests as outlined in our policies because public health needs dictated that we do as much testing as possible. But as the process has matured, we have helped increase the number of authorized tests, and we have adapted some of our policies to best serve the public need.
Today, if evidence arises that raises questions about a particular test’s reliability, we will take appropriate action to protect consumers from inaccurate tests. This is a dynamic process that is continually being informed by new data and evidence.
We’ve used a similar dynamic process in the search for therapeutic treatments and vaccines.
We are working closely with partners throughout the government and academia, and with drug and vaccine developers to explore, expedite, and incentivize the development of these products.
More than 90 drugs are being studied, and FDA is actively working with numerous vaccine sponsors, including three sponsors who have announced they have vaccine candidates that are now in clinical trials in the U.S. More than 144 clinical trials have been initiated for therapeutic agents, with hundreds more in the pipeline. We don’t have a cure or vaccine yet, but we’re on our way, at unprecedented speed.
Ultimately, of course, the way we’ll eventually defeat this virus is with a vaccine. FDA is working closely to provide technical assistance to federal partners, vaccine developers, researchers, manufacturers, and experts across the globe and exploring all possible options to advance the most efficient and timely development of vaccines, while at the same time maintaining regulatory independence.
Communicating and Educating
There is much more to do going forward, and that includes research, exploration and discovery, and communicating what we know.
As the country starts to reopen, it’s essential that the public understands what they need to do to continue to protect themselves. There has been a proliferation of information, and misinformation, on the internet and in other sources. Consumers need to understand that this virus is still with us and that we, as individuals and communities working together, need to take steps to continue to contain its spread.
The FDA has an important part to play in communicating public information to all populations in the U.S. FDA has increased outreach by developing and disseminating COVID-19 health education materials for consumers in multiple languages to diverse communities and the public overall. Everyone should have a clear understanding of why hand-washing and social distancing remain essential. Consumers need to think about how to shop for food safely. People need to know when to call their doctors and when to ask about getting tested. Health care professionals need to know how to manage their patients in this new environment, and how best to apply telemedicine, the use of which is rapidly accelerating.
I want the FDA to serve as a national resource for the public and health care community. I regard educating the public and providing accurate, reliable, up-to-date information as not just an Agency priority, but one of my own personal responsibilities as Commissioner. I will be out in public and in the media talking about how individuals can help us contain and conquer this virus.
I believe my personal experience with being self-quarantined will make me a better communicator. Being quarantined for 14 days in May was certainly no fun, but because we at FDA were already functioning very effectively virtually, I was able to continue to be fully engaged, and provide direction and leadership. And it made me even more focused on making sure consumers have all the information they need about self-protection.
We now need to look forward. A major strength of the FDA is not just in our response to a crisis, but in our ability to learn from the work we do and apply that experience in the future.
As this pandemic evolved, it was clear that some FDA processes needed to be adjusted to accommodate the urgency of the pandemic. I think the entire FDA team has now seen first-hand that we need to look at some of our processes and policies. I have instructed my staff to identify the lessons learned from this pandemic and what adjustments may be needed, not just to manage this or future emergencies, but to make FDA itself more efficient in carrying out our regulatory responsibilities.
I am committed to making sure that some of the lessons learned from managing this pandemic will lead to permanent improvements at the FDA in processes and policies.
For example, in facilitating the development of new treatments, we streamlined some of our processes.
We have taken a fresh look at how clinical trials should be designed and conducted. In a pandemic we knew we needed to get answers more quickly. For instance, early on, the FDA, National Institutes of Health, and industry worked together to facilitate the implementation of a “master protocol” that can be used in multiple clinical trials and allows for the study of more than one promising new drug for COVID-19 at a time. And we have used expanded access to meet the needs of patients who are not eligible or who are unable to participate in randomized clinical trials.
Many of the permanent changes that we will implement really represent an acceleration of where we were headed before. For example, the concept of decentralized clinical trials, in which trial procedures are conducted near the patient’s home and through use of local health care providers or local laboratories has been discussed before, and laid the foundation for some of the trials for COVID-19 products.
Another area where our pre-COVID work has informed our response to the pandemic involves the use of Real World Evidence (RWE).
In recent years, the agency has taken steps to leverage modern, rigorous analyses of real-world data—such as data from electronic health records, insurance claims, patient registries and lab results.
As the pandemic brought an urgency to these efforts, the FDA advanced collaborations with public and private partners to collect and analyze a variety of real-world data sources, using our Sentinel system and other resources.
Evaluation of real-world data has the potential to provide a wealth of rapid, actionable information to better understand disease symptoms, describe and measure immunity, and use available medical product supplies to help mitigate potential shortages. These data can also inform ongoing work to evaluate potential therapies, vaccines or diagnostics for COVID-19. The more experience we have with real world evidence, the more confidence we will have in using it for product decisions.
I mention real world evidence, but in reality, we have so many examples of how lessons learned from the pandemic will affect FDA in the future.
To the extent that the innovations and adaptations we implemented during the pandemic crisis worked and would be appropriate to implement outside of a pandemic situation, we will incorporate them into standard FDA procedures. And to the extent that we identified unnecessary barriers, we will remove them. This is one of my top priorities. Permanent change where needed will take place, and will make FDA an even stronger agency.
As I mentioned before, anything that enables quicker reviews and authorizations we will seek to make permanent.
But make no mistake. We will not cut corners on safety or effectiveness. I said this before, and I say it again. Good science as the basis for decision making has been a hallmark of my career, and is a value that I hold deeply. The American public must have confidence in the products regulated by the FDA.
Speed is important, but so are safety, accuracy and effectiveness.
FDA’s commitment to good science and rigorous data is unwavering, even as we look at how we can learn from this pandemic.
I am hopeful that this is a once-in-a-lifetime experience for all of us. An unprecedented historic event that has required an unprecedented response from us and everyone around the world.
That said, I am pleased that throughout this crisis the rest of the FDA’s work has continued, with relatively few interruptions. New drugs and devices have been authorized. Our food safety surveillance has adapted and our outbreak response resources have been maintained. Our oversight of tobacco products, including e-cigarettes, has gone on. The Agency has measured up to the challenge in all ways.
And we are well positioned as we move into a new phase, that is, transitioning back to what has come to be known as the “new normal.” Our staff has done a phenomenal job of adapting to this new normal. And I am confident that they are ready to deal with any additional upcoming challenges.
I will close with something I’ve seen reaffirmed time and time again over the past few months. That is the essential role that the FDA plays in consumer protection and beyond in advancing public health.
Before coming to the FDA, I had heard about the extraordinary dedication of the agency’s workforce. Working side by side with my colleagues in response to this pandemic, I’ve seen that characterization validated over and over.
It is my great honor to serve with so many highly skilled and committed professionals. And the American people can be assured that this agency is working around the clock for them, doing whatever is necessary to fulfill our mission to protect and promote the health of the American public.
I encourage you all to stay safe, aware, and focused as we continue to respond to the challenges of this public health emergency.
Search the United Nations
- Policy and Funding
- Recover Better
- Disability Inclusion
- Secretary-General
- Financing for Development
- ACT-Accelerator
- Member States
- Health and Wellbeing
- Policy and Guidance
- Vaccination
- COVID-19 Medevac
- i-Seek (requires login)
- Awake at Night podcast

“Now is the time for unity”
About the author, antónio guterres.
António Guterres is the ninth Secretary-General of the United Nations, who took office on 1st January 2017.
The Covid-19 pandemic is one of the most dangerous challenges this world has faced in our lifetime. It is above all a human crisis with severe health and socio-economic consequences.
The World Health Organization, with thousands of its staff, is on the front lines, supporting Member States and their societies, especially the most vulnerable among them, with guidance, training, equipment and concrete life-saving services as they fight the virus.
The World Health Organization must be supported, as it is absolutely critical to the world’s efforts to win the war against Covid-19.
I witnessed first-hand the courage and determination of WHO staff when I visited the Democratic Republic of the Congo last year, where WHO staff are working in precarious conditions and very dangerous remote locations as they fight the deadly Ebola virus. It has been a remarkable success for WHO that no new cases of Ebola have been registered in months.
It is my belief that the World Health Organization must be supported, as it is absolutely critical to the world’s efforts to win the war against Covid-19.
This virus is unprecedented in our lifetime and requires an unprecedented response. Obviously, in such conditions, it is possible that the same facts have had different readings by different entities. Once we have finally turned the page on this epidemic, there must be a time to look back fully to understand how such a disease emerged and spread its devastation so quickly across the globe, and how all those involved reacted to the crisis. The lessons learned will be essential to effectively address similar challenges, as they may arise in the future.
But now is not that time. Now is the time for unity, for the international community to work together in solidarity to stop this virus and its shattering consequences.

S7-Episode 2: Bringing Health to the World
“You see, we're not doing this work to make ourselves feel better. That sort of conventional notion of what a do-gooder is. We're doing this work because we are totally convinced that it's not necessary in today's wealthy world for so many people to be experiencing discomfort, for so many people to be experiencing hardship, for so many people to have their lives and their livelihoods imperiled.”
Dr. David Nabarro has dedicated his life to global health. After a long career that’s taken him from the horrors of war torn Iraq, to the devastating aftermath of the Indian Ocean tsunami, he is still spurred to action by the tremendous inequalities in global access to medical care.
“The thing that keeps me awake most at night is the rampant inequities in our world…We see an awful lot of needless suffering.”
:: David Nabarro interviewed by Melissa Fleming

Brazilian ballet pirouettes during pandemic
Ballet Manguinhos, named for its favela in Rio de Janeiro, returns to the stage after a long absence during the COVID-19 pandemic. It counts 250 children and teenagers from the favela as its performers. The ballet group provides social support in a community where poverty, hunger and teen pregnancy are constant issues.

Radio journalist gives the facts on COVID-19 in Uzbekistan
The pandemic has put many people to the test, and journalists are no exception. Coronavirus has waged war not only against people's lives and well-being but has also spawned countless hoaxes and scientific falsehoods.
- Newsletters
Site search
- Israel-Hamas war
- Home Planet
- 2024 election
- Supreme Court
- All explainers
- Future Perfect
Filed under:
Read these 12 moving essays about life during coronavirus
Artists, novelists, critics, and essayists are writing the first draft of history.
Share this story
- Share this on Facebook
- Share this on Twitter
- Share this on Reddit
- Share All sharing options
Share All sharing options for: Read these 12 moving essays about life during coronavirus
/cdn.vox-cdn.com/uploads/chorus_image/image/66606035/1207638131.jpg.0.jpg)
The world is grappling with an invisible, deadly enemy, trying to understand how to live with the threat posed by a virus . For some writers, the only way forward is to put pen to paper, trying to conceptualize and document what it feels like to continue living as countries are under lockdown and regular life seems to have ground to a halt.
So as the coronavirus pandemic has stretched around the world, it’s sparked a crop of diary entries and essays that describe how life has changed. Novelists, critics, artists, and journalists have put words to the feelings many are experiencing. The result is a first draft of how we’ll someday remember this time, filled with uncertainty and pain and fear as well as small moments of hope and humanity.
At the New York Review of Books, Ali Bhutto writes that in Karachi, Pakistan, the government-imposed curfew due to the virus is “eerily reminiscent of past military clampdowns”:
Beneath the quiet calm lies a sense that society has been unhinged and that the usual rules no longer apply. Small groups of pedestrians look on from the shadows, like an audience watching a spectacle slowly unfolding. People pause on street corners and in the shade of trees, under the watchful gaze of the paramilitary forces and the police.
His essay concludes with the sobering note that “in the minds of many, Covid-19 is just another life-threatening hazard in a city that stumbles from one crisis to another.”
Writing from Chattanooga, novelist Jamie Quatro documents the mixed ways her neighbors have been responding to the threat, and the frustration of conflicting direction, or no direction at all, from local, state, and federal leaders:
Whiplash, trying to keep up with who’s ordering what. We’re already experiencing enough chaos without this back-and-forth. Why didn’t the federal government issue a nationwide shelter-in-place at the get-go, the way other countries did? What happens when one state’s shelter-in-place ends, while others continue? Do states still under quarantine close their borders? We are still one nation, not fifty individual countries. Right?
Award-winning photojournalist Alessio Mamo, quarantined with his partner Marta in Sicily after she tested positive for the virus, accompanies his photographs in the Guardian of their confinement with a reflection on being confined :
The doctors asked me to take a second test, but again I tested negative. Perhaps I’m immune? The days dragged on in my apartment, in black and white, like my photos. Sometimes we tried to smile, imagining that I was asymptomatic, because I was the virus. Our smiles seemed to bring good news. My mother left hospital, but I won’t be able to see her for weeks. Marta started breathing well again, and so did I. I would have liked to photograph my country in the midst of this emergency, the battles that the doctors wage on the frontline, the hospitals pushed to their limits, Italy on its knees fighting an invisible enemy. That enemy, a day in March, knocked on my door instead.
In the New York Times Magazine, deputy editor Jessica Lustig writes with devastating clarity about her family’s life in Brooklyn while her husband battled the virus, weeks before most people began taking the threat seriously:
At the door of the clinic, we stand looking out at two older women chatting outside the doorway, oblivious. Do I wave them away? Call out that they should get far away, go home, wash their hands, stay inside? Instead we just stand there, awkwardly, until they move on. Only then do we step outside to begin the long three-block walk home. I point out the early magnolia, the forsythia. T says he is cold. The untrimmed hairs on his neck, under his beard, are white. The few people walking past us on the sidewalk don’t know that we are visitors from the future. A vision, a premonition, a walking visitation. This will be them: Either T, in the mask, or — if they’re lucky — me, tending to him.
Essayist Leslie Jamison writes in the New York Review of Books about being shut away alone in her New York City apartment with her 2-year-old daughter since she became sick:
The virus. Its sinewy, intimate name. What does it feel like in my body today? Shivering under blankets. A hot itch behind the eyes. Three sweatshirts in the middle of the day. My daughter trying to pull another blanket over my body with her tiny arms. An ache in the muscles that somehow makes it hard to lie still. This loss of taste has become a kind of sensory quarantine. It’s as if the quarantine keeps inching closer and closer to my insides. First I lost the touch of other bodies; then I lost the air; now I’ve lost the taste of bananas. Nothing about any of these losses is particularly unique. I’ve made a schedule so I won’t go insane with the toddler. Five days ago, I wrote Walk/Adventure! on it, next to a cut-out illustration of a tiger—as if we’d see tigers on our walks. It was good to keep possibility alive.
At Literary Hub, novelist Heidi Pitlor writes about the elastic nature of time during her family’s quarantine in Massachusetts:
During a shutdown, the things that mark our days—commuting to work, sending our kids to school, having a drink with friends—vanish and time takes on a flat, seamless quality. Without some self-imposed structure, it’s easy to feel a little untethered. A friend recently posted on Facebook: “For those who have lost track, today is Blursday the fortyteenth of Maprilay.” ... Giving shape to time is especially important now, when the future is so shapeless. We do not know whether the virus will continue to rage for weeks or months or, lord help us, on and off for years. We do not know when we will feel safe again. And so many of us, minus those who are gifted at compartmentalization or denial, remain largely captive to fear. We may stay this way if we do not create at least the illusion of movement in our lives, our long days spent with ourselves or partners or families.
Novelist Lauren Groff writes at the New York Review of Books about trying to escape the prison of her fears while sequestered at home in Gainesville, Florida:
Some people have imaginations sparked only by what they can see; I blame this blinkered empiricism for the parks overwhelmed with people, the bars, until a few nights ago, thickly thronged. My imagination is the opposite. I fear everything invisible to me. From the enclosure of my house, I am afraid of the suffering that isn’t present before me, the people running out of money and food or drowning in the fluid in their lungs, the deaths of health-care workers now growing ill while performing their duties. I fear the federal government, which the right wing has so—intentionally—weakened that not only is it insufficient to help its people, it is actively standing in help’s way. I fear we won’t sufficiently punish the right. I fear leaving the house and spreading the disease. I fear what this time of fear is doing to my children, their imaginations, and their souls.
At ArtForum , Berlin-based critic and writer Kristian Vistrup Madsen reflects on martinis, melancholia, and Finnish artist Jaakko Pallasvuo’s 2018 graphic novel Retreat , in which three young people exile themselves in the woods:
In melancholia, the shape of what is ending, and its temporality, is sprawling and incomprehensible. The ambivalence makes it hard to bear. The world of Retreat is rendered in lush pink and purple watercolors, which dissolve into wild and messy abstractions. In apocalypse, the divisions established in genesis bleed back out. My own Corona-retreat is similarly soft, color-field like, each day a blurred succession of quarantinis, YouTube–yoga, and televized press conferences. As restrictions mount, so does abstraction. For now, I’m still rooting for love to save the world.
At the Paris Review , Matt Levin writes about reading Virginia Woolf’s novel The Waves during quarantine:
A retreat, a quarantine, a sickness—they simultaneously distort and clarify, curtail and expand. It is an ideal state in which to read literature with a reputation for difficulty and inaccessibility, those hermetic books shorn of the handholds of conventional plot or characterization or description. A novel like Virginia Woolf’s The Waves is perfect for the state of interiority induced by quarantine—a story of three men and three women, meeting after the death of a mutual friend, told entirely in the overlapping internal monologues of the six, interspersed only with sections of pure, achingly beautiful descriptions of the natural world, a day’s procession and recession of light and waves. The novel is, in my mind’s eye, a perfectly spherical object. It is translucent and shimmering and infinitely fragile, prone to shatter at the slightest disturbance. It is not a book that can be read in snatches on the subway—it demands total absorption. Though it revels in a stark emotional nakedness, the book remains aloof, remote in its own deep self-absorption.
In an essay for the Financial Times, novelist Arundhati Roy writes with anger about Indian Prime Minister Narendra Modi’s anemic response to the threat, but also offers a glimmer of hope for the future:
Historically, pandemics have forced humans to break with the past and imagine their world anew. This one is no different. It is a portal, a gateway between one world and the next. We can choose to walk through it, dragging the carcasses of our prejudice and hatred, our avarice, our data banks and dead ideas, our dead rivers and smoky skies behind us. Or we can walk through lightly, with little luggage, ready to imagine another world. And ready to fight for it.
From Boston, Nora Caplan-Bricker writes in The Point about the strange contraction of space under quarantine, in which a friend in Beirut is as close as the one around the corner in the same city:
It’s a nice illusion—nice to feel like we’re in it together, even if my real world has shrunk to one person, my husband, who sits with his laptop in the other room. It’s nice in the same way as reading those essays that reframe social distancing as solidarity. “We must begin to see the negative space as clearly as the positive, to know what we don’t do is also brilliant and full of love,” the poet Anne Boyer wrote on March 10th, the day that Massachusetts declared a state of emergency. If you squint, you could almost make sense of this quarantine as an effort to flatten, along with the curve, the distinctions we make between our bonds with others. Right now, I care for my neighbor in the same way I demonstrate love for my mother: in all instances, I stay away. And in moments this month, I have loved strangers with an intensity that is new to me. On March 14th, the Saturday night after the end of life as we knew it, I went out with my dog and found the street silent: no lines for restaurants, no children on bicycles, no couples strolling with little cups of ice cream. It had taken the combined will of thousands of people to deliver such a sudden and complete emptiness. I felt so grateful, and so bereft.
And on his own website, musician and artist David Byrne writes about rediscovering the value of working for collective good , saying that “what is happening now is an opportunity to learn how to change our behavior”:
In emergencies, citizens can suddenly cooperate and collaborate. Change can happen. We’re going to need to work together as the effects of climate change ramp up. In order for capitalism to survive in any form, we will have to be a little more socialist. Here is an opportunity for us to see things differently — to see that we really are all connected — and adjust our behavior accordingly. Are we willing to do this? Is this moment an opportunity to see how truly interdependent we all are? To live in a world that is different and better than the one we live in now? We might be too far down the road to test every asymptomatic person, but a change in our mindsets, in how we view our neighbors, could lay the groundwork for the collective action we’ll need to deal with other global crises. The time to see how connected we all are is now.
The portrait these writers paint of a world under quarantine is multifaceted. Our worlds have contracted to the confines of our homes, and yet in some ways we’re more connected than ever to one another. We feel fear and boredom, anger and gratitude, frustration and strange peace. Uncertainty drives us to find metaphors and images that will let us wrap our minds around what is happening.
Yet there’s no single “what” that is happening. Everyone is contending with the pandemic and its effects from different places and in different ways. Reading others’ experiences — even the most frightening ones — can help alleviate the loneliness and dread, a little, and remind us that what we’re going through is both unique and shared by all.
Will you support Vox today?
We believe that everyone deserves to understand the world that they live in. That kind of knowledge helps create better citizens, neighbors, friends, parents, and stewards of this planet. Producing deeply researched, explanatory journalism takes resources. You can support this mission by making a financial gift to Vox today. Will you join us?
We accept credit card, Apple Pay, and Google Pay. You can also contribute via
Next Up In Culture
Sign up for the newsletter today, explained.
Understand the world with a daily explainer plus the most compelling stories of the day.
Thanks for signing up!
Check your inbox for a welcome email.
Oops. Something went wrong. Please enter a valid email and try again.

How a bunch of Redditors made GameStop’s stock soar

Sen. Bob Menendez’s corruption trial, explained

Pig kidney transplants are cool. They shouldn’t be necessary.

8 surprising reasons to stop hating cicadas and start worshipping them

The 9 worst court decisions since Trump remade the federal judiciary

Speed limits are too darn high
- Share full article
Advertisement
Supported by
current events
12 Ideas for Writing Through the Pandemic With The New York Times
A dozen writing projects — including journals, poems, comics and more — for students to try at home.

By Natalie Proulx
The coronavirus has transformed life as we know it. Schools are closed, we’re confined to our homes and the future feels very uncertain. Why write at a time like this?
For one, we are living through history. Future historians may look back on the journals, essays and art that ordinary people are creating now to tell the story of life during the coronavirus.
But writing can also be deeply therapeutic. It can be a way to express our fears, hopes and joys. It can help us make sense of the world and our place in it.
Plus, even though school buildings are shuttered, that doesn’t mean learning has stopped. Writing can help us reflect on what’s happening in our lives and form new ideas.
We want to help inspire your writing about the coronavirus while you learn from home. Below, we offer 12 projects for students, all based on pieces from The New York Times, including personal narrative essays, editorials, comic strips and podcasts. Each project features a Times text and prompts to inspire your writing, as well as related resources from The Learning Network to help you develop your craft. Some also offer opportunities to get your work published in The Times, on The Learning Network or elsewhere.
We know this list isn’t nearly complete. If you have ideas for other pandemic-related writing projects, please suggest them in the comments.
In the meantime, happy writing!
Journaling is well-known as a therapeutic practice , a tool for helping you organize your thoughts and vent your emotions, especially in anxiety-ridden times. But keeping a diary has an added benefit during a pandemic: It may help educate future generations.
In “ The Quarantine Diaries ,” Amelia Nierenberg spoke to Ady, an 8-year-old in the Bay Area who is keeping a diary. Ms. Nierenberg writes:
As the coronavirus continues to spread and confine people largely to their homes, many are filling pages with their experiences of living through a pandemic. Their diaries are told in words and pictures: pantry inventories, window views, questions about the future, concerns about the present. Taken together, the pages tell the story of an anxious, claustrophobic world on pause. “You can say anything you want, no matter what, and nobody can judge you,” Ady said in a phone interview earlier this month, speaking about her diary. “No one says, ‘scaredy-cat.’” When future historians look to write the story of life during coronavirus, these first-person accounts may prove useful. “Diaries and correspondences are a gold standard,” said Jane Kamensky, a professor of American History at Harvard University and the faculty director of the Schlesinger Library at the Radcliffe Institute. “They’re among the best evidence we have of people’s inner worlds.”
You can keep your own journal, recording your thoughts, questions, concerns and experiences of living through the coronavirus pandemic.
Not sure what to write about? Read the rest of Ms. Nierenberg’s article to find out what others around the world are recording. If you need more inspiration, here are a few writing prompts to get you started:
How has the virus disrupted your daily life? What are you missing? School, sports, competitions, extracurricular activities, social plans, vacations or anything else?
What effect has this crisis had on your own mental and emotional health?
What changes, big or small, are you noticing in the world around you?
For more ideas, see our writing prompts . We post a new one every school day, many of them now related to life during the coronavirus.
You can write in your journal every day or as often as you like. And if writing isn’t working for you right now, try a visual, audio or video diary instead.
2. Personal Narrative
As you write in your journal, you’ll probably find that your life during the pandemic is full of stories, whether serious or funny, angry or sad. If you’re so inspired, try writing about one of your experiences in a personal narrative essay.
Here’s how Mary Laura Philpott begins her essay, “ This Togetherness Is Temporary, ” about being quarantined with her teenage children:
Get this: A couple of months ago, I quit my job in order to be home more. Go ahead and laugh at the timing. I know. At the time, it was hitting me that my daughter starts high school in the fall, and my son will be a senior. Increasingly they were spending their time away from me at school, with friends, and in the many time-intensive activities that make up teenage lives. I could feel the clock ticking, and I wanted to spend the minutes I could — the minutes they were willing to give me, anyway — with them, instead of sitting in front of a computer at night and on weekends in order to juggle a job as a bookseller, a part-time gig as a television host, and a book deadline. I wanted more of them while they were still living in my house. Now here we are, all together, every day. You’re supposed to be careful what you wish for, but come on. None of us saw this coming.
Personal narratives are short, powerful stories about meaningful life experiences, big or small. Read the rest of Ms. Philpott’s essay to see how she balances telling the story of a specific moment in time and reflecting on what it all means in the larger context of her life.
To help you identify the moments that have been particularly meaningful, difficult, comical or strange during this pandemic, try responding to one of our writing prompts related to the coronavirus:
Holidays and Birthdays Are Moments to Come Together. How Are You Adapting During the Pandemic?
Has Your School Switched to Remote Learning? How Is It Going So Far?
Is the Coronavirus Pandemic Bringing Your Extended Family Closer Together?
How Is the Coronavirus Outbreak Affecting Your Life?
Another option? Use any of the images in our Picture Prompt series to inspire you to write about a memory from your life.
Related Resource: Writing Curriculum | Unit 1: Teach Narrative Writing With The New York Times

People have long turned to creative expression in times of crisis. During the coronavirus pandemic, artists are continuing to illustrate , play music , dance , perform — and write poetry .
That’s what Dr. Elizabeth Mitchell, an emergency room doctor in Boston, did after a long shift treating coronavirus patients. Called “ The Apocalypse ,” her poem begins like this:
This is the apocalypse A daffodil has poked its head up from the dirt and opened sunny arms to bluer skies yet I am filled with dark and anxious dread as theaters close as travel ends and grocery stores display their empty rows where toilet paper liquid bleach and bags of flour stood in upright ranks.
Read the rest of Dr. Mitchell’s poem and note the lines, images and metaphors that speak to you. Then, tap into your creative side by writing a poem inspired by your own experience of the pandemic.
Need inspiration? Try writing a poem in response to one of our Picture Prompts . Or, you can create a found poem using an article from The Times’s coronavirus outbreak coverage . If you have access to the print paper, try making a blackout poem instead.
Related Resources: 24 Ways to Teach and Learn About Poetry With The New York Times Reader Idea | How the Found Poem Can Inspire Teachers and Students Alike
4. Letter to the Editor
Have you been keeping up with the news about the coronavirus? What is your reaction to it?
Make your voice heard by writing a letter to the editor about a recent Times article, editorial, column or Opinion essay related to the pandemic. You can find articles in The Times’s free coronavirus coverage or The Learning Network’s coronavirus resources for students . And, if you’re a high school student, your school can get you free digital access to The New York Times from now until July 6.
To see examples, read the letters written by young people in response to recent headlines in “ How the Young Deal With the Coronavirus .” Here’s what Addie Muller from San Jose, Calif., had to say about the Opinion essay “ I’m 26. Coronavirus Sent Me to the Hospital ”:
As a high school student and a part of Generation Z, I’ve been less concerned about getting Covid-19 and more concerned about spreading it to more vulnerable populations. While I’ve been staying at home and sheltering in place (as was ordered for the state of California), many of my friends haven’t been doing the same. I know people who continue going to restaurants and have been treating the change in education as an extended spring break and excuse to spend more time with friends. I fear for my grandparents and parents, but this article showed me that we should also fear for ourselves. I appreciated seeing this article because many younger people seem to feel invincible. The fact that a healthy 26-year-old can be hospitalized means that we are all capable of getting the virus ourselves and spreading it to others. I hope that Ms. Lowenstein continues spreading her story and that she makes a full recovery soon.
As you read, note some of the defining features of a letter to the editor and what made these good enough to publish. For more advice, see these tips from Thomas Feyer, the letters editor at The Times, about how to write a compelling letter. They include:
Write briefly and to the point.
Be prepared to back up your facts with evidence.
Write about something off the beaten path.
Publishing Opportunity: When you’re ready, submit your letter to The New York Times.
5. Editorial
Maybe you have more to say than you can fit in a 150-word letter to the editor. If that’s the case, try writing an editorial about something you have a strong opinion about related to the coronavirus. What have you seen that has made you upset? Proud? Appreciative? Scared?
In “ Surviving Coronavirus as a Broke College Student ,” Sydney Goins, a senior English major at the University of Georgia, writes about the limited options for students whose colleges are now closed. Her essay begins:
College was supposed to be my ticket to financial security. My parents were the first ones to go to college in their family. My grandpa said to my mom, “You need to go to college, so you don’t have to depend on a man for money.” This same mentality was passed on to me as well. I had enough money to last until May— $1,625 to be exact — until the coronavirus ruined my finances. My mom works in human resources. My dad is a project manager for a mattress company. I worked part time at the university’s most popular dining hall and lived in a cramped house with three other students. I don’t have a car. I either walked or biked a mile to attend class. I have student debt and started paying the accrued interest last month. I was making it work until the coronavirus shut down my college town. At first, spring break was extended by two weeks with the assumption that campus would open again in late March, but a few hours after that email, all 26 colleges in the University System of Georgia canceled in-person classes and closed integral parts of campus.
Read the rest of Ms. Goins’s essay. What is her argument? How does she support it? How is it relevant to her life and the world?
Then, choose a topic related to the pandemic that you care about and write an editorial that asserts an opinion and backs it up with solid reasoning and evidence.
Not sure where to start? Try responding to some of our recent argumentative writing prompts and see what comes up for you. Here are a few we’ve asked students so far:
Should Schools Change How They Grade Students During the Pandemic?
What Role Should Celebrities Have During the Coronavirus Crisis?
Is It Immoral to Increase the Price of Goods During a Crisis?
Or, consider essential questions about the pandemic and what they tell us about our world today: What weaknesses is the coronavirus exposing in our society? How can we best help our communities right now? What lessons can we learn from this crisis? See more here.
As an alternative to a written essay, you might try creating a video Op-Ed instead, like Katherine Oung’s “ Coronavirus Racism Infected My High School. ”
Publishing Opportunity: Submit your final essay to our Student Editorial Contest , open to middle school and high school students ages 10-19, until April 21. Please be sure to read all the rules and guidelines before submitting.
Related Resource: An Argumentative-Writing Unit for Students Doing Remote Learning
Are games, television, music, books, art or movies providing you with a much-needed distraction during the pandemic? What has been working for you that you would recommend to others? Or, what would you caution others to stay away from right now?
Share your opinions by writing a review of a piece of art or culture for other teenagers who are stuck at home. You might suggest TV shows, novels, podcasts, video games, recipes or anything else. Or, try something made especially for the coronavirus era, like a virtual architecture tour , concert or safari .
As a mentor text, read Laura Cappelle’s review of French theater companies that have rushed to put content online during the coronavirus outbreak, noting how she tailors her commentary to our current reality:
The 17th-century philosopher Blaise Pascal once wrote: “The sole cause of people’s unhappiness is that they do not know how to stay quietly in their rooms.” Yet at a time when much of the world has been forced to hunker down, French theater-makers are fighting to fill the void by making noise online.
She continues:
Under the circumstances, it would be churlish to complain about artists’ desire to connect with audiences in some fashion. Theater, which depends on crowds gathering to watch performers at close quarters, is experiencing significant loss and upheaval, with many stagings either delayed indefinitely or canceled outright. But a sampling of stopgap offerings often left me underwhelmed.
To get inspired you might start by responding to our related Student Opinion prompt with your recommendations. Then turn one of them into a formal review.
Related Resource: Writing Curriculum | Unit 2: Analyzing Arts, Criticizing Culture: Writing Reviews With The New York Times
7. How-to Guide
Being stuck at home with nowhere to go is the perfect time to learn a new skill. What are you an expert at that you can you teach someone?
The Times has created several guides that walk readers through how to do something step-by-step, for example, this eight-step tutorial on how to make a face mask . Read through the guide, noting how the author breaks down each step into an easily digestible action, as well as how the illustrations support comprehension.
Then, create your own how-to guide for something you could teach someone to do during the pandemic. Maybe it’s a recipe you’ve perfected, a solo sport you’ve been practicing, or a FaceTime tutorial for someone who’s never video chatted before.
Whatever you choose, make sure to write clearly so anyone anywhere could try out this new skill. As an added challenge, include an illustration, photo, or audio or video clip with each step to support the reader’s understanding.
Related Resource: Writing Curriculum | Unit 4: Informational Writing
8. 36 Hours Column
For nearly two decades, The Times has published a weekly 36 Hours column , giving readers suggestions for how to spend a weekend in cities all over the globe.
While traveling for fun is not an option now, the Travel section decided to create a special reader-generated column of how to spend a weekend in the midst of a global pandemic. The result? “ 36 Hours in … Wherever You Are .” Here’s how readers suggest spending a Sunday morning:
8 a.m. Changing routines Make small discoveries. To stretch my legs during the lockdown, I’ve been walking around the block every day, and I’ve started to notice details that I’d never seen before. Like the fake, painted window on the building across the road, or the old candle holders that were once used as part of the street lighting. When the quarantine ends, I hope we don’t forget to appreciate what’s been on a doorstep all along. — Camilla Capasso, Modena, Italy 10:30 a.m. Use your hands Undertake the easiest and most fulfilling origami project of your life by folding 12 pieces of paper and building this lovely star . Modular origami has been my absolute favorite occupational therapy since I was a restless child: the process is enthralling and soothing. — Laila Dib, Berlin, Germany 12 p.m. Be isolated, together Check on neighbors on your block or floor with an email, text or phone call, or leave a card with your name and contact information. Are they OK? Do they need something from the store? Help with an errand? Food? Can you bring them a hot dish or home-baked bread? This simple act — done carefully and from a safe distance — palpably reduces our sense of fear and isolation. I’ve seen the faces of some neighbors for the first time. Now they wave. — Jim Carrier, Burlington, Vt.
Read the entire article. As you read, consider: How would this be different if it were written by teenagers for teenagers?
Then, create your own 36 Hours itinerary for teenagers stuck at home during the pandemic with ideas for how to spend the weekend wherever they are.
The 36 Hours editors suggest thinking “within the spirit of travel, even if many of us are housebound.” For example: an album or a song playlist; a book or movie that transports you; a particular recipe you love; or a clever way to virtually connect with family and friends. See more suggestions here .
Related Resources: Reader Idea | 36 Hours in Your Hometown 36 Hours in Learning: Creating Travel Itineraries Across the Curriculum
9. Photo Essay

Daily life looks very different now. Unusual scenes are playing out in homes, parks, grocery stores and streets across the country.
In “ New York Was Not Designed for Emptiness ,” New York Times photographers document what life in New York City looks like amid the pandemic. It begins:
The lights are still on in Times Square. Billboards blink and storefronts shine in neon. If only there were an audience for this spectacle. But the thoroughfares have been abandoned. The energy that once crackled along the concrete has eased. The throngs of tourists, the briskly striding commuters, the honking drivers have mostly skittered away. In their place is a wistful awareness that plays across all five boroughs: Look how eerie our brilliant landscape has become. Look how it no longer bustles. This is not the New York City anyone signed up for.
Read the rest of the essay and view the photos. As you read, note the photos or lines in the text that grab your attention most. Why do they stand out to you?
What does the pandemic look like where you live? Create your own photo essay, accompanied by a written piece, that illustrates your life now. In your essay, consider how you can communicate a particular theme or message about life during the pandemic through both your photos and words, like in the article you read.
Publishing Opportunity: The International Center of Photography is collecting a virtual archive of images related to the coronavirus pandemic. Learn how to submit yours here.
10. Comic Strip
Sometimes, words alone just won’t do. Visual mediums, like comics, have the advantage of being able to express emotion, reveal inner monologues, and explain complex subjects in ways that words on their own seldom can.
If anything proves this point, it is the Opinion section’s ongoing visual diary, “ Art in Isolation .” Scroll through this collection to see clever and poignant illustrations about life in these uncertain times. Read the comic “ Finding Connection When Home Alone ” by Gracey Zhang from this collection. As you read, note what stands out to you about the writing and illustrations. What lessons could they have for your own piece?
Then, create your own comic strip, modeled after the one you read, that explores some aspect of life during the pandemic. You can sketch and color your comic with paper and pen, or use an online tool like MakeBeliefsComix.com .
Need inspiration? If you’re keeping a quarantine journal, as we suggested above, you might create a graphic story based on a week of your life, or just a small part of it — like the meals you ate, the video games you played, or the conversations you had with friends over text. For more ideas, check out our writing prompts related to the coronavirus.
Related Resource: From Superheroes to Syrian Refugees: Teaching Comics and Graphic Novels With Resources From The New York Times
11. Podcast
Modern Love Podcast: In the Midst of the Coronavirus Pandemic, People Share Their Love Stories
Are you listening to any podcasts to help you get through the pandemic? Are they keeping you up-to-date on the news? Offering advice? Or just helping you escape from it all?
Create your own five-minute podcast segment that responds to the coronavirus in some way.
To get an idea of the different genres and formats your podcast could take, listen to one or more of these five-minute clips from three New York Times podcast episodes related to the coronavirus:
“ The Daily | Voices of the Pandemic ” (1:15-6:50)
“ Still Processing | A Pod From Both Our Houses ” (0:00-4:50)
“ Modern Love | In the Midst of the Coronavirus Pandemic, People Share Their Love Stories ” (1:30-6:30)
Use these as models for your own podcast. Consider the different narrative techniques they use to relate an experience of the pandemic — interviews, nonfiction storytelling and conversation — as well as how they create an engaging listening experience.
Need ideas for what to talk about? You might try translating any of the writing projects above into podcast form. Or turn to our coronavirus-related writing prompts for inspiration.
Publishing Opportunity: Submit your finished five-minute podcast to our Student Podcast Contest , which is open through May 19. Please read all the rules and guidelines before submitting.
Related Resource: Project Audio: Teaching Students How to Produce Their Own Podcasts
12. Revise and Edit
“It doesn’t matter how good you think you are as a writer — the first words you put on the page are a first draft,” Harry Guinness writes in “ How to Edit Your Own Writing .”
Editing your work may seem like something you do quickly — checking for spelling mistakes just before you turn in your essay — but Mr. Guinness argues it’s a project in its own right:
The time you put into editing, reworking and refining turns your first draft into a second — and then into a third and, if you keep at it, eventually something great. The biggest mistake you can make as a writer is to assume that what you wrote the first time through was good enough.
Read the rest of the article for a step-by-step guide to editing your own work. Then, revise one of the pieces you have written, following Mr. Guinness’s advice.
Publishing Opportunity: When you feel like your piece is “something great,” consider submitting it to one of the publishing opportunities we’ve suggested above. Or, see our list of 70-plus places that publish teenage writing and art to find more.
Natalie Proulx joined The Learning Network as a staff editor in 2017 after working as an English language arts teacher and curriculum writer. More about Natalie Proulx
MINI REVIEW article
Covid-19: emergence, spread, possible treatments, and global burden.

- 1 Department of Pharmacology, Manipal College of Pharmaceutical Sciences, Manipal Academy of Higher Education, Manipal, India
- 2 Department of Health Sciences, School of Education and Health, Cape Breton University, Sydney, NS, Canada
The Coronavirus (CoV) is a large family of viruses known to cause illnesses ranging from the common cold to acute respiratory tract infection. The severity of the infection may be visible as pneumonia, acute respiratory syndrome, and even death. Until the outbreak of SARS, this group of viruses was greatly overlooked. However, since the SARS and MERS outbreaks, these viruses have been studied in greater detail, propelling the vaccine research. On December 31, 2019, mysterious cases of pneumonia were detected in the city of Wuhan in China's Hubei Province. On January 7, 2020, the causative agent was identified as a new coronavirus (2019-nCoV), and the disease was later named as COVID-19 by the WHO. The virus spread extensively in the Wuhan region of China and has gained entry to over 210 countries and territories. Though experts suspected that the virus is transmitted from animals to humans, there are mixed reports on the origin of the virus. There are no treatment options available for the virus as such, limited to the use of anti-HIV drugs and/or other antivirals such as Remdesivir and Galidesivir. For the containment of the virus, it is recommended to quarantine the infected and to follow good hygiene practices. The virus has had a significant socio-economic impact globally. Economically, China is likely to experience a greater setback than other countries from the pandemic due to added trade war pressure, which have been discussed in this paper.
Introduction
Coronaviridae is a family of viruses with a positive-sense RNA that possess an outer viral coat. When looked at with the help of an electron microscope, there appears to be a unique corona around it. This family of viruses mainly cause respiratory diseases in humans, in the forms of common cold or pneumonia as well as respiratory infections. These viruses can infect animals as well ( 1 , 2 ). Up until the year 2003, coronavirus (CoV) had attracted limited interest from researchers. However, after the SARS (severe acute respiratory syndrome) outbreak caused by the SARS-CoV, the coronavirus was looked at with renewed interest ( 3 , 4 ). This also happened to be the first epidemic of the 21st century originating in the Guangdong province of China. Almost 10 years later, there was a MERS (Middle East respiratory syndrome) outbreak in 2012, which was caused by the MERS-CoV ( 5 , 6 ). Both SARS and MERS have a zoonotic origin and originated from bats. A unique feature of these viruses is the ability to mutate rapidly and adapt to a new host. The zoonotic origin of these viruses allows them to jump from host to host. Coronaviruses are known to use the angiotensin-converting enzyme-2 (ACE-2) receptor or the dipeptidyl peptidase IV (DPP-4) protein to gain entry into cells for replication ( 7 – 10 ).
In December 2019, almost seven years after the MERS 2012 outbreak, a novel Coronavirus (2019-nCoV) surfaced in Wuhan in the Hubei region of China. The outbreak rapidly grew and spread to neighboring countries. However, rapid communication of information and the increasing scale of events led to quick quarantine and screening of travelers, thus containing the spread of the infection. The major part of the infection was restricted to China, and a second cluster was found on a cruise ship called the Diamond Princess docked in Japan ( 11 , 12 ).
The new virus was identified to be a novel Coronavirus and was thus initially named 2019-nCoV; later, it was renamed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) ( 13 ), and the disease it causes is now referred to as Coronavirus Disease-2019 (COVID-19) by the WHO. The virus was suspected to have begun its spread in the Huanan seafood wholesale market in the Wuhan region. It is possible that an animal that was carrying the virus was brought into or sold in the market, causing the spread of the virus in the crowded marketplace. One of the first claims made was in an article published in the Journal of Medical Virology ( 14 ), which identified snakes as the possible host. A second possibility was that pangolins could be the wild host of SARS-CoV-2 ( 15 ), though the most likely possibility is that the virus originated from bats ( 13 , 16 – 19 ). Increasing evidence and experts are now collectively concluding the virus had a natural origin in bats, as with previous such respiratory viruses ( 2 , 20 – 24 ).
Similarly, SARS and MERS were also suspected to originate from bats. In the case of MERS, the dromedary camel is an intermediate host ( 5 , 10 ). Bats have been known to harbor coronaviruses for quite some time now. Just as in the case of avian flu, SARS, MERS, and possibly even HIV, with increasing selection and ecological pressure due to human activities, the virus made the jump from animal to man. Humans have been encroaching increasingly into forests, and this is true over much of China, as in Africa. Combined with additional ecological pressure due to climate change, such zoonotic spillovers are now more common than ever. It is likely that the next disease X will also have such an origin ( 25 ). We have learned the importance of identification of the source organism due to the Ebola virus pandemic. Viruses are unstable organisms genetically, constantly mutating by genetic shift or drift. It is not possible to predict when a cross-species jump may occur and when a seemingly harmless variant form of the virus may turn into a deadly strain. Such an incident occurred in Reston, USA, with the Reston virus ( 26 ), an alarming reminder of this possibility. The identification of the original host helps us to contain future spreads as well as to learn about the mechanism of transmission of viruses. Until the virus is isolated from a wild animal host, in this case, mostly bats, the zoonotic origin will remain hypothetical, though likely. It should further be noted that the virus has acquired several mutations, as noted by a group in China, indicating that there are more than two strains of the virus, which may have had an impact on its pathogenicity. However, this claim remains unproven, and many experts have argued otherwise; data proving this are not yet available ( 27 ). A similar finding was reported from Italy and India independently, where they found two strains ( 28 , 29 ). These findings need to be further cross-verified by similar analyses globally. If true, this finding could effectively explain why some nations are more affected than others.
Transmission
When the spread of COVID-19 began ( Figure 1 ), the virus appeared to be contained within China and the cruise ship “Diamond Princess,” which formed the major clusters of the virus. However, as of April 2020, over 210 countries and territories are affected by the virus, with Europe, the USA, and Iran forming the new cluster of the virus. The USA ( Figure 2 ) has the highest number of confirmed COVID-19 cases, whereas India and China, despite being among the most population-dense countries in the world, have managed to constrain the infection rate by the implementation of a complete lockdown with arrangements in place to manage the confirmed cases. Similarly, the UK has also managed to maintain a low curve of the graph by implementing similar measures, though it was not strictly enforced. Reports have indicated that the presence of different strains or strands of the virus may have had an effect on the management of the infection rate of the virus ( 27 – 29 ). The disease is spread by droplet transmission. As of April 2020, the total number of infected individuals stands at around 3 million, with ~200,000 deaths and more than 1 million recoveries globally ( 30 , 34 ). The virus thus has a fatality rate of around 2% and an R 0 of 3 based on current data. However, a more recent report from the CDC, Atlanta, USA, claims that the R 0 could be as high as 5.7 ( 35 ). It has also been observed from data available from China and India that individuals likely to be infected by the virus from both these countries belong to the age groups of 20–50 years ( 36 , 37 ). In both of these countries, the working class mostly belongs to this age group, making exposure more likely. Germany and Singapore are great examples of countries with a high number of cases but low fatalities as compared to their immediate neighbors. Singapore is one of the few countries that had developed a detailed plan of action after the previous SARS outbreak to deal with a similar situation in the future, and this worked in their favor during this outbreak. Both countries took swift action after the outbreak began, with Singapore banning Chinese travelers and implementing screening and quarantine measures at a time when the WHO recommended none. They ordered the elderly and the vulnerable to strictly stay at home, and they ensured that lifesaving equipment and large-scale testing facilities were available immediately ( 38 , 39 ). Germany took similar measures by ramping up testing capacity quite early and by ensuring that all individuals had equal opportunity to get tested. This meant that young, old, and at-risk people all got tested, thus ensuring positive results early during disease progression and that most cases were mild like in Singapore, thus maintaining a lower death percentage ( 40 ). It allowed infected individuals to be identified and quarantined before they even had symptoms. Testing was carried out at multiple labs, reducing the load and providing massive scale, something which countries such as the USA did quite late and India restricted to select government and private labs. The German government also banned large gatherings and advocated social distancing to further reduce the spread, though unlike India and the USA, this was done quite late. South Korea is another example of how a nation has managed to contain the spread and transmission of the infection. South Korea and the USA both reported their first COVID-19 cases on the same day; however, the US administration downplayed the risks of the disease, unlike South Korean officials, who constantly informed their citizens about the developments of the disease using the media and a centralized messaging system. They also employed the Trace, Test, and Treat protocol to identify and isolate patients fast, whereas the USA restricted this to patients with severe infection and only later broadened this criterion, like many European countries as well as India. Unlike the USA, South Korea also has universal healthcare, ensuring free diagnostic testing.

Figure 1 . Timeline of COVID-19 progression ( 30 – 32 ).

Figure 2 . Total confirmed COVID 19 cases as of May 2020 ( 33 ).
The main mode of transmission of 2019-nCoV is human to human. As of now, animal-to-human transfer has not yet been confirmed. Asymptomatic carriers of the virus are at major risk of being superinfectors with this disease, as all those infected may not develop the disease ( 41 ). This is a concern that has been raised by nations globally, with the Indian government raising concerns on how to identify and contain asymptomatic carriers, who could account for 80% of those infected ( 42 ). Since current resources are directed towards understanding the hospitalized individuals showing symptoms, there is still a vast amount of information about asymptomatic individuals that has yet to be studied. For example, some questions that need to be answered include: Do asymptomatic individuals develop the disease at any point in time at all? Do they eventually develop antibodies? How long do they shed the virus for? Can any tissue of these individuals store the virus in a dormant state? Asymptomatic transmission is a gray area that encompasses major unknowns in COVID-19.
The main route of human-to-human transmission is by droplets, which are generated during coughing, talking, or sneezing and are then inhaled by a healthy individual. They can also be indirectly transmitted to a person when they land on surfaces that are touched by a healthy individual who may then touch their nose, mouth, or eyes, allowing the virus entry into the body. Fomites are also a common issue in such diseases ( 43 ).
Aerosol-based transmission of the virus has not yet been confirmed ( 43 ). Stool-based transmission via the fecal-oral route may also be possible since the SARS-CoV-2 has been found in patient feces ( 44 , 45 ). Some patients with COVID-19 tend to develop diarrhea, which can become a major route of transmission if proper sanitation and personal hygiene needs are not met. There is no evidence currently available to suggest intrauterine vertical transmission of the disease in pregnant women ( 46 ).
More investigation is necessary of whether climate has played any role in the containment of the infection in countries such as India, Singapore, China, and Israel, as these are significantly warmer countries as compared with the UK, the USA, and Canada ( Figure 2 ). Ideally, a warm climate should prevent the virus from surviving for longer periods of time on surfaces, reducing transmissibility.
Pathophysiology
On gaining entry via any of the mucus membranes, the single-stranded RNA-based virus enters the host cell using type 2 transmembrane serine protease (TMPRSS2) and ACE2 receptor protein, leading to fusion and endocytosis with the host cell ( 47 – 49 ). The uncoated RNA is then translated, and viral proteins are synthesized. With the help of RNA-dependant RNA polymerase, new RNA is produced for the new virions. The cell then undergoes lysis, releasing a load of new virions into the patients' body. The resultant infection causes a massive release of pro-inflammatory cytokines that causes a cytokine storm.
Clinical Presentation
The clinical presentation of the disease resembles beta coronavirus infections. The virus has an incubation time of 2–14 days, which is the reason why most patients suspected to have the illness or contact with an individual having the illness remain in quarantine for the said amount of time. Infection with SARS-CoV-2 causes severe pneumonia, intermittent fever, and cough ( 50 , 51 ). Symptoms of rhinorrhoea, pharyngitis, and sneezing have been less commonly seen. Patients often develop acute respiratory distress syndrome within 2 days of hospital admission, requiring ventilatory support. It has been observed that during this phase, the mortality tends to be high. Chest CT will show indicators of pneumonia and ground-glass opacity, a feature that has helped to improve the preliminary diagnosis ( 51 ). The primary method of diagnosis for SARS-CoV-2 is with the help of PCR. For the PCR testing, the US CDC recommends testing for the N gene, whereas the Chinese CDC recommends the use of ORF lab and N gene of the viral genome for testing. Some also rely on the radiological findings for preliminary screening ( 52 ). Additionally, immunodiagnostic tests based on the presence of antibodies can also play a role in testing. While the WHO recommends the use of these tests for research use, many countries have pre-emptively deployed the use of these tests in the hope of ramping up the rate and speed of testing ( 52 – 54 ). Later, they noticed variations among the results, causing them to stop the use of such kits; there was also debate among the experts about the sensitivity and specificity of the tests. For immunological tests, it is beneficial to test for antibodies against the virus produced by the body rather than to test for the presence of the viral proteins, since the antibodies can be present in larger titers for a longer span of time. However, the cross-reactivity of these tests with other coronavirus antibodies is something that needs verification. Biochemical parameters such as D-dimer, C-reactive protein, and variations in neutrophil and lymphocyte counts are some other parameters that can be used to make a preliminary diagnosis; however, these parameters vary in a number of diseases and thus cannot be relied upon conclusively ( 51 ). Patients with pre-existing diseases such as asthma or similar lung disorder are at higher risk, requiring life support, as are those with other diseases such as diabetes, hypertension, or obesity. Those above the age of 60 have displayed the highest mortality rate in China, a finding that is mirrored in other nations as well ( Figure 3 ) ( 55 ). If we cross-verify these findings with the population share that is above the age of 70, we find that Italy, the United Kingdom, Canada, and the USA have one of the highest elderly populations as compared to countries such as India and China ( Figure 4 ), and this also reflects the case fatality rates accordingly ( Figure 5 ) ( 33 ). This is a clear indicator that aside from comorbidities, age is also an independent risk factor for death in those infected by COVID-19. Also, in the US, it was seen that the rates of African American deaths were higher. This is probably due to the fact that the prevalence of hypertension and obesity in this community is higher than in Caucasians ( 56 , 57 ). In late April 2020, there are also claims in the US media that young patients in the US with COVID-19 may be at increased risk of stroke; however, this is yet to be proven. We know that coagulopathy is a feature of COVID-19, and thus stroke is likely in this condition ( 58 , 59 ). The main cause of death in COVID-19 patients was acute respiratory distress due to the inflammation in the linings of the lungs caused by the cytokine storm, which is seen in all non-survival cases and in respiratory failure. The resultant inflammation in the lungs, served as an entry point of further infection, associated with coagulopathy end-organ failure, septic shock, and secondary infections leading to death ( 60 – 63 ).

Figure 3 . Case fatality rate by age in selected countries as of April 2020 ( 33 ).

Figure 4 . Case fatality rate in selected countries ( 33 ).

Figure 5 . Population share above 70 years of age ( 33 ).
For COVID-19, there is no specific treatment available. The WHO announced the organization of a trial dubbed the “Solidarity” clinical trial for COVID-19 treatments ( 64 ). This is an international collaborative study that investigates the use of a few prime candidate drugs for use against COVID-19, which are discussed below. The study is designed to reduce the time taken for an RCT by over 80%. There are over 1087 studies ( Supplementary Data 1 ) for COVID-19 registered at clinicaltrials.gov , of which 657 are interventional studies ( Supplementary Data 2 ) ( 65 ). The primary focus of the interventional studies for COVID-19 has been on antimalarial drugs and antiviral agents ( Table 1 ), while over 200 studies deal with the use of different forms of oxygen therapy. Most trials focus on improvement of clinical status, reduction of viral load, time to improvement, and reduction of mortality rates. These studies cover both severe and mild cases.

Table 1 . List of therapeutic drugs under study for COVID-19 as per clinical trials registered under clinicaltrials.gov .
Use of Antimalarial Drugs Against SARS-CoV-2
The use of chloroquine for the treatment of corona virus-based infection has shown some benefit in the prevention of viral replication in the cases of SARS and MERS. However, it was not validated on a large scale in the form of a randomized control trial ( 50 , 66 – 68 ). The drugs of choice among antimalarials are Chloroquine (CQ) and Hydroxychloroquine (HCQ). The use of CQ for COVID-19 was brought to light by the Chinese, especially by the publication of a letter to the editor of Bioscience Trends by Gao et al. ( 69 ). The letter claimed that several studies found CQ to be effective against COVID-19; however, the letter did not provide many details. Immediately, over a short span of time, interest in these two agents grew globally. Early in vitro data have revealed that chloroquine can inhibit the viral replication ( 70 , 71 ).
HCQ and CQ work by raising the pH of the lysosome, the cellular organelle that is responsible for phagocytic degradation. Its function is to combine with cell contents that have been phagocytosed and break them down eventually, in some immune cells, as a downstream process to display some of the broken proteins as antigens, thus further enhancing the immune recruitment against an antigen/pathogen. The drug was to be administered alone or with azithromycin. The use of azithromycin may be advocated by the fact that it has been seen previously to have some immunomodulatory role in airway-related disease. It appears to reduce the release of pro-inflammatory cytokines in respiratory illnesses ( 72 ). However, HCQ and azithromycin are known to have a major drug interaction when co-administered, which increases the risk of QT interval prolongation ( 73 ). Quinine-based drugs are known to have adverse effects such as QT prolongation, retinal damage, hypoglycemia, and hemolysis of blood in patients with G-6-PD deficiency ( 66 ). Several preprints, including, a metanalysis now indicate that HCQ may have no benefit for severe or critically ill patients who have COVID-19 where the outcome is need for ventilation or death ( 74 , 75 ). As of April 21, 2020, after having pre-emptively recommended their use for SARS-CoV-2 infection, the US now advocates against the use of these two drugs based on the new data that has become available.
Use of Antiviral Drugs Against SARS-CoV-2
The antiviral agents are mainly those used in the case of HIV/AIDS, these being Lopinavir and Ritonavir. Other agents such as nucleoside analogs like Favipiravir, Ribavirin, Remdesivir, and Galidesivir have been tested for possible activity in the prevention of viral RNA synthesis ( 76 ). Among these drugs, Lopinavir, Ritonavir, and Remdesivir are listed in the Solidarity trial by the WHO.
Remdesivir is a nucleotide analog for adenosine that gets incorporated into the viral RNA, hindering its replication and causing chain termination. This agent was originally developed for Ebola Virus Disease ( 77 ). A study was conducted with rhesus macaques infected with SARS-CoV-2 ( 78 ). In that study, after 12 h of infection, the monkeys were treated with either Remdesivir or vehicle. The drug showed good distribution in the lungs, and the animals treated with the drug showed a better clinical score than the vehicle group. The radiological findings of the study also indicated that the animals treated with Remdesivir have less lung damage. There was a reduction in viral replication but not in virus shedding. Furthermore, there were no mutations found in the RNA polymerase sequences. A randomized clinical control study that became available in late April 2020 ( 79 ), having 158 on the Remdesivir arm and 79 on the placebo arm, found that Remdesivir reduced the time to recovery in the Remdesivir-treated arm to 11 days, while the placebo-arm recovery time was 15 days. Though this was not found to be statistically significant, the agent provided a basis for further studies. The 28-days mortality was found to be similar for both groups. This has now provided us with a basis on which to develop future molecules. The study has been supported by the National Institute of Health, USA. The authors of the study advocated for more clinical trials with Remdesivir with a larger population. Such larger studies are already in progress, and their results are awaited. Remdesivir is currently one of the drugs that hold most promise against COVID-19.
An early trial in China with Lopinavir and Ritonavir showed no benefit compared with standard clinical care ( 80 ). More studies with this drug are currently underway, including one in India ( 81 , 82 ).
Use of Convalescent Patient Plasma
Another possible option would be the use of serum from convalescent individuals, as this is known to contain antibodies that can neutralize the virus and aid in its elimination. This has been tried previously for other coronavirus infections ( 83 ). Early emerging case reports in this aspect look promising compared to other therapies that have been tried ( 84 – 87 ). A report from China indicates that five patients treated with plasma recovered and were eventually weaned off ventilators ( 84 ). They exhibited reductions in fever and viral load and improved oxygenation. The virus was not detected in the patients after 12 days of plasma transfusion. The US FDA has provided detailed recommendations for investigational COVID-19 Convalescent Plasma use ( 88 ). One of the benefits of this approach is that it can also be used for post-exposure prophylaxis. This approach is now beginning to be increasingly adopted in other countries, with over 95 trials registered on clinicaltrials.gov alone, of which at least 75 are interventional ( 89 ). The use of convalescent patient plasma, though mostly for research purposes, appears to be the best and, so far, the only successful option for treatment available.
From a future perspective, the use of monoclonal antibodies for the inhibition of the attachment of the virus to the ACE-2 receptor may be the best bet. Aside from this, ACE-2-like molecules could also be utilized to attach and inactivate the viral proteins, since inhibition of the ACE-2 receptor would not be advisable due to its negative repercussions physiologically. In the absence of drug regimens and a vaccine, the treatment is symptomatic and involves the use of non-invasive ventilation or intubation where necessary for respiratory failure patients. Patients that may go into septic shock should be managed as per existing guidelines with hemodynamic support as well as antibiotics where necessary.
The WHO has recommended that simple personal hygiene practices can be sufficient for the prevention of spread and containment of the disease ( 90 ). Practices such as frequent washing of soiled hands or the use of sanitizer for unsoiled hands help reduce transmission. Covering of mouth while sneezing and coughing, and disinfection of surfaces that are frequently touched, such as tabletops, doorknobs, and switches with 70% isopropyl alcohol or other disinfectants are broadly recommended. It is recommended that all individuals afflicted by the disease, as well as those caring for the infected, wear a mask to avoid transmission. Healthcare works are advised to wear a complete set of personal protective equipment as per WHO-provided guidelines. Fumigation of dormitories, quarantine rooms, and washing of clothes and other fomites with detergent and warm water can help get rid of the virus. Parcels and goods are not known to transmit the virus, as per information provided by the WHO, since the virus is not able to survive sufficiently in an open, exposed environment. Quarantine of infected individuals and those who have come into contact with an infected individual is necessary to further prevent transmission of the virus ( 91 ). Quarantine is an age-old archaic practice that continues to hold relevance even today for disease containment. With the quarantine being implemented on such a large scale in some countries, taking the form of a national lockdown, the question arises of its impact on the mental health of all individuals. This topic needs to be addressed, especially in countries such as India and China, where it is still a matter of partial taboo to talk about it openly within the society.
In India, the Ministry of Ayurveda, Yoga, and Naturopathy, Unani, Siddha and Homeopathy (AYUSH), which deals with the alternative forms of medicine, issued a press release that the homeopathic, drug Arsenicum album 30, can be taken on an empty stomach for 3 days to provide protection against the infection ( 92 ). It also provided a list of herbal drugs in the same press release as per Ayurvedic and Unani systems of medicine that can boost the immune system to deal with the virus. However, there is currently no evidence to support the use of these systems of medicine against COVID-19, and they need to be tested.
The prevention of the disease with the use of a vaccine would provide a more viable solution. There are no vaccines available for any of the coronaviruses, which includes SARS and MERS. The development of a vaccine, however, is in progress at a rapid pace, though it could take about a year or two. As of April 2020, no vaccine has completed the development and testing process. A popular approach has been with the use of mRNA-based vaccine ( 93 – 96 ). mRNA vaccines have the advantage over conventional vaccines in terms of production, since they can be manufactured easily and do not have to be cultured, as a virus would need to be. Alternative conventional approaches to making a vaccine against SARS-CoV-2 would include the use of live attenuated virus as well as using the isolated spike proteins of the virus. Both of these approaches are in progress for vaccine development ( 97 ). Governments across the world have poured in resources and made changes in their legislation to ensure rapid development, testing, and deployment of a vaccine.
Barriers to Treatment
Lack of transparency and poor media relations.
The lack of government transparency and poor reporting by the media have hampered the measures that could have been taken by healthcare systems globally to deal with the COVID-19 threat. The CDC, as well as the US administration, downplayed the threat and thus failed to stock up on essential supplies, ventilators, and test kits. An early warning system, if implemented, would have caused borders to be shut and early lockdowns. The WHO also delayed its response in sounding the alarm regarding the severity of the outbreak to allow nations globally to prepare for a pandemic. Singapore is a prime example where, despite the WHO not raising concerns and banning travel to and from China, a country banned travelers and took early measures, thus managing the outbreak quite well. South Korea is another example of how things may have played out had those measures by agencies been taken with transparency. Increased transparency would have allowed the healthcare sector to better prepare and reduced the load of patients they had to deal with, helping flatten the curve. The increased patient load and confusion among citizens arising from not following these practices has proved to be a barrier to providing effective treatments to patients with the disease elsewhere in the world.
Lack of Preparedness and Protocols
Despite the previous SARS outbreak teaching us important lessons and providing us with data on a potential outbreak, many nations did not take the important measures needed for a future outbreak. There was no allocation of sufficient funds for such an event. Many countries experienced severe lack of PPE, and the lockdown precautions hampered the logistics of supply and manufacturing of such essential equipment. Singapore and South Korea had protocols in place and were able to implement them at a moment's notice. The spurt of cases that Korea experienced was managed well, providing evidence to this effect. The lack of preparedness and lack of protocol in other nations has resulted in confusion as to how the treatment may be administered safely to the large volume of patients while dealing with diagnostics. Both of these factors have limited the accessibility to healthcare services due to sheer volume.
Socio-Economic Impact
During the SARS epidemic, China faced an economic setback, and experts were unsure if any recovery would be made. However, the global and domestic situation was then in China's favor, as it had a lower debt, allowing it to make a speedy recovery. This is not the case now. Global experts have a pessimistic outlook on the outcome of this outbreak ( 98 ). The fear of COVID-19 disease, lack of proper understanding of the dangers of the virus, and the misinformation spread on the social media ( 99 ) have caused a breakdown of the economic flow globally ( 100 ). An example of this is Indonesia, where a great amount of fear was expressed in responses to a survey when the nation was still free of COVID-19 ( 101 ). The pandemic has resulted in over 2.6 billion people being put under lockdown. This lockdown and the cancellation of the lunar year celebration has affected business at the local level. Hundreds of flights have been canceled, and tourism globally has been affected. Japan and Indonesia are estimated to lose over 2.44 billion dollars due to this ( 102 , 103 ). Workers are not able to work in factories, transportation in all forms is restricted, and goods are not produced or moved. The transport of finished products and raw materials out of China is low. The Economist has published US stock market details indicating that companies in the US that have Chinese roots fell, on average, 5 points on the stock market as compared to the S&P 500 index ( 104 ). Companies such as Starbucks have had to close over 4,000 outlets due to the outbreak as a precaution. Tech and pharma companies are at higher risk since they rely on China for the supply of raw materials and active pharmaceutical ingredients. Paracetamol, for one, has reported a price increase of over 40% in India ( 104 – 106 ). Mass hysteria in the market has caused selling of shares of these companies, causing a tumble in the Indian stock market. Though long-term investors will not be significantly affected, short-term traders will find themselves in soup. Politically, however, this has further bolstered support for world leaders in countries such as India, Germany, and the UK, who are achieving good approval ratings, with citizens being satisfied with the government's approach. In contrast, the ratings of US President Donald Trump have dropped due to the manner in which the COVID-19 pandemic was handled. These minor impacts may be of temporary significance, and the worst and direct impact will be on China itself ( 107 – 109 ), as the looming trade war with the USA had a negative impact on the Chinese and Asian markets. The longer production of goods continues to remain suspended, the more adversely it will affect the Chinese economy and the global markets dependent on it ( 110 ). If this disease is not contained, more and more lockdowns by multiple nations will severely affect the economy and lead to many social complications.
The appearance of the 2019 Novel Coronavirus has added and will continue to add to our understanding of viruses. The pandemic has once again tested the world's preparedness for dealing with such outbreaks. It has provided an outlook on how a massive-scale biological event can cause a socio-economic disturbance through misinformation and social media. In the coming months and years, we can expect to gain further insights into SARS-CoV-2 and COVID-19.
Author Contributions
KN: conceptualization. RK, AA, JM, and KN: investigation. RK and AA: writing—original draft preparation. KN, PN, and JM: writing—review and editing. KN: supervision.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to acknowledge the contributions made by Dr. Piya Paul Mudgal, Assistant Professor, Manipal Institute of Virology, Manipal Academy of Higher Education towards inputs provided by her during the drafting of the manuscript.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2020.00216/full#supplementary-material
Supplementary Data 1, 2. List of all studies registered for COVID-19 on clinicaltrials.gov .
1. McIntosh K, Dees JH, Becker WB, Kapikian AZ, Chanock RM. Recovery in tracheal organ cultures of novel viruses from patients with respiratory disease. Proc Natl Acad Sci USA. (1967) 57:933–40. doi: 10.1073/pnas.57.4.933
PubMed Abstract | CrossRef Full Text | Google Scholar
2. Esper F, Weibel C, Ferguson D, Landry ML, Kahn JS. Evidence of a novel human coronavirus that is associated with respiratory tract disease in infants and young children. J Infect Dis. (2005) 191:492–8. doi: 10.1086/428138
3. Stöhr K. A multicentre collaboration to investigate the cause of severe acute respiratory syndrome. Lancet. (2003) 361:1730–3. doi: 10.1016/S0140-6736(03)13376-4
4. Peiris JSM, Lai ST, Poon LLM, Guan Y, Yam LYC, Lim W, et al. Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet. (2003) 361:1319–25. doi: 10.1016/S0140-6736(03)13077-2
5. Zumla A, Hui DS, Perlman S. Middle East respiratory syndrome. Lancet. (2015) 386:995–1007. doi: 10.1016/S0140-6736(15)60454-8
6. Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus ADME, Fouchier RAM. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. (2012) 367:1814–20. doi: 10.1056/NEJMoa1211721
7. Perlman S, Netland J. Coronaviruses post-SARS: update on replication and pathogenesis. Nat Rev Microbiol. (2009) 7:439–50. doi: 10.1038/nrmicro2147
8. Li W, Moore MJ, Vasllieva N, Sui J, Wong SK, Berne MA, et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature. (2003) 426:450–4. doi: 10.1038/nature02145
9. Ge X-Y, Li J-L, Yang X-L, Chmura AA, Zhu G, Epstein JH, et al. Isolation and characterization of a bat SARS-like coronavirus that uses the ACE2 receptor. Nature. (2013) 503:535–8. doi: 10.1038/nature12711
10. Wang M, Hu Z. Bats as animal reservoirs for the SARS coronavirus: Hypothesis proved after 10 years of virus hunting. Virol Sin. (2013) 28:315–7. doi: 10.1007/s12250-013-3402-x
11. Diamond Princess Cruise Ship in Japan Confirms 99 New Coronavirus Cases | World news | The Guardian. Available online at: https://www.theguardian.com/world/2020/feb/17/coronavirus-japan-braces-for-hundreds-more-cases-as-another-china-city-locked-down (accessed February 17, 2020).
Google Scholar
12. Diamond Princess Coronavirus & Quarantine Updates - Notices & Advisories - Princess Cruises. Available online at: https://www.princess.com/news/notices_and_advisories/notices/diamond-princess-update.html (accessed February 17, 2020).
13. Gorbalenya AE, Baker SC, Baric RS, Groot RJ, de Drosten C, Gulyaeva AA, et al. The species severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. (2020) 5:536–44. doi: 10.1038/s41564-020-0695-z
14. Ji W, Wang W, Zhao X, Zai J, Li X. Homologous recombination within the spike glycoprotein of the newly identified coronavirus may boost cross-species transmission from snake to human. J Med Virol . (2020) 7:jmv.25682. doi: 10.1002/jmv.25682
15. Cyranoski D. Did pangolins spread the China coronavirus to people? Nature . (2020) doi: 10.1038/d41586-020-00364-2
CrossRef Full Text | Google Scholar
16. Lu R, Zhao X, Li J, Niu P, Yang B, Wu H, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. (2020) 395:565–74. doi: 10.1016/S0140-6736(20)30251-8
17. Wassenaar TM, Zou Y. 2019_nCoV: Rapid classification of betacoronaviruses and identification of traditional Chinese medicine as potential origin of zoonotic coronaviruses. Lett Appl Microbiol. (2020) 70:324–48. doi: 10.1111/lam.13285
18. Velavan TP, Meyer CG. The Covid-19 epidemic. Trop Med Int Heal . (2020) 25:278–80. doi: 10.1111/tmi.13383
19. Guarner J. Three Emerging Coronaviruses in Two Decades. Am J Clin Pathol . (2020) 153:420–21. doi: 10.1093/ajcp/aqaa029
20. Li W, Shi Z, Yu M, Ren W, Smith C, Epstein JH, et al. Bats are natural reservoirs of SARS-like coronaviruses. Science. (2005) 310:676–9. doi: 10.1126/science.1118391
21. Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. (2020) 579:270–3. doi: 10.1038/s41586-020-2012-7
22. Menachery VD, Yount BL, Debbink K, Agnihothram S, Gralinski LE, Plante JA, et al. A SARS-like cluster of circulating bat coronaviruses shows potential for human emergence. Nat Med. (2015) 21:1508–13. doi: 10.1038/nm.3985
23. COVID-19 Coronavirus Epidemic has a Natural Origin—ScienceDaily. Available online at: https://www.sciencedaily.com/releases/2020/03/200317175442.htm (accessed April 22, 2020).
24. Andersen KG, Rambaut A, Lipkin WI, Holmes EC, Garry RF. The proximal origin of SARS-CoV-2. Nat Med . (2020) 26:450–2. doi: 10.1038/s41591-020-0820-9
25. Prioritizing Diseases for Research and Development in Emergency Contexts. Available online at: https://www.who.int/activities/prioritizing-diseases-for-research-and-development-in-emergency-contexts (accessed April 22, 2020).
26. Albariño CG, Guerrero LW, Jenks HM, Chakrabarti AK, Ksiazek TG, Rollin PE, et al. Insights into Reston virus spillovers and adaption from virus whole genome sequences. PLoS ONE. (2017) 12:e0178224. doi: 10.1371/journal.pone.0178224
27. Yao H, Lu X, Chen Q, Xu K, Chen Y, Cheng L, et al. Patient-derived mutations impact pathogenicity of SARS-CoV-2. medRxiv. (2020). doi: 10.2139/ssrn.3578153
28. Stefanelli P, Faggioni G, Lo Presti A, Fiore S, Marchi A, Benedetti E, et al. Whole genome and phylogenetic analysis of two SARS-CoV-2 strains isolated in Italy in January and February 2020: additional clues on multiple introductions and further circulation in Europe. Eurosurveillance. (2020) 25:2000305. doi: 10.2807/1560-7917.ES.2020.25.13.2000305
29. Yadav P, Potdar V, Choudhary M, Nyayanit D, Agrawal M, Jadhav S, et al. Full-genome sequences of the first two SARS-CoV-2 viruses from India. Indian J Med Res. (2020) 151:200–9. doi: 10.4103/ijmr.IJMR_663_20
30. WHO | Coronavirus disease 2019 (COVID-19) Situation Report – 26. Beijing (2020). Available online at: http://www.nhc.gov.cn/xcs/yqtb/list_gzbd.shtml (accessed February 16, 2020).
31. WHO | Middle East Respiratory Syndrome Coronavirus (MERS-CoV). World Health Organization (2020).
32. WHO | Summary of Probable SARS Cases With Onset of Illness From 1 November 2002 to 31 July 2003. World Health Organization (2015).
33. Worldometer. Coronavirus cases. Worldometer. (2020) 1−22.
34. Update on the Outbreak of New Coronavirus Pneumonia as of 24 hours on 15 February. Beijing (2020). Available online at: http://www.nhc.gov.cn/xcs/yqtb/list_gzbd.shtml (accessed February 16, 2020).
35. Sanche S, Lin YT, Xu C, Romero-Severson E, Hengartner N, Ke R. High contagiousness and rapid spread of severe acute respiratory syndrome coronavirus 2. Emerg Infect Dis. (2020) 26. doi: 10.3201/eid2607.200282
36. 83% of India's Coronavirus Patients Are Below the Age of 50: Health ministry data - India News. Available online at: https://www.indiatoday.in/india/story/83-of-india-s-coronavirus-patients-are-below-the-age-of-50-health-ministry-data-1663314-2020-04-04 (accessed April 23, 2020).
37. 42% of Coronavirus Patients in 21-40 age bracket: Govt. Available online at: https://economictimes.indiatimes.com/news/politics-and-nation/42-of-coronavirus-patients-in-21-40-age-bracket-govt/articleshow/74987254.cms (accessed April 23, 2020).
38. Why COVID-19 Case Counts Are so Low in Singapore Hong Kong and Taiwan | Advisory Board Daily Briefing. Available online at: https://www.advisory.com/daily-briefing/2020/03/19/asian-countries (accessed April 29, 2020).
39. Coronavirus: Why so Few Deaths Among Singapore's 14000 Covid-19 Infections? | South China Morning Post. Available online at: https://www.scmp.com/weekasia/health-environment/article/3081772/coronavirus-why-so-few-deaths-among-singapores-14000 (accessed April 29, 2020).
40. Stafford N. Covid-19: Why Germany's case fatality rate seems so low. BMJ. (2020) 7:369. doi: 10.1136/bmj.m1395
41. Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission of 2019-NCOV infection from an asymptomatic contact in Germany. N Engl J Med . (2020) 382:970–1. doi: 10.1056/NEJMc2001468
42. Coronavirus pandemic | 80% of COVID-19 Cases Either Asymptomatic or Show Mild Symptoms. Health ministry - Moneycontrol.com. Available online at: https://www.moneycontrol.com/news/india/coronavirus-pandemic-80-of-covid-19-cases-either-asymptomatic-or-show-mild-symptoms-health-ministry-5170631.html (accessed April 24, 2020).
43. WHO | Q&A on Coronaviruses. Available online at: https://www.who.int/news-room/q-a-detail/q-a-coronaviruses (accessed February 16, 2020).
44. Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H, et al. First Case of 2019 Novel Coronavirus in the United States. N Engl J Med . (2020) 382:929–36. doi: 10.1056/NEJMoa2001191
45. Yeo C, Kaushal S, Yeo D. Enteric involvement of coronaviruses: is faecal–oral transmission of SARS-CoV-2 possible? Lancet Gastroenterol Hepatol. (2020) 5:335–37. doi: 10.1016/S2468-1253(20)30048-0
46. Chen H, Guo J, Wang C, Luo F, Yu X, Zhang W, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. (2020) 395:809–15. doi: 10.1016/S0140-6736(20)30360-3
47. Fehr AR, Perlman S. Coronaviruses: An overview of their replication and pathogenesis. In: Coronaviruses: Methods and Protocols (New York: Springer), 1–23. doi: 10.1007/978-1-4939-2438-7_1
48. Chen Y, Liu Q, Guo D. Emerging coronaviruses: Genome structure, replication, and pathogenesis. J Med Virol. (2020) 92:418–23. doi: 10.1002/jmv.25681
49. Hoffmann M, Kleine-Weber H, Schroeder S, Mü MA, Drosten C, Pö S. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. (2020) 181:271–80. doi: 10.1016/j.cell.2020.02.052
50. Cheng VCC, Chan JFW, To KKW, Yuen KY. Clinical management and infection control of SARS: Lessons learned. Antiviral Res. (2013) 100:407–19. doi: 10.1016/j.antiviral.2013.08.016
51. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
52. Udugama B, Kadhiresan P, Kozlowski HN, Malekjahani A, Osborne M, Li VYC, et al. Diagnosing COVID-19: the disease and tools for detection. ACS Nano . (2020) 14:3822–35. doi: 10.1021/acsnano.0c02624
53. Testing, | CDC,. Available online at: https://www.cdc.gov/coronavirus/2019-ncov/testing/index.html (accessed April 29, 2020).
54. Advice on the Use of Point-of-Care Immunodiagnostic Tests for COVID-19. Available online at: https://www.who.int/news-room/commentaries/detail/advice-on-the-use-of-point-of-care-immunodiagnostic-tests-for-covid-19 (accessed April 29, 2020).
55. Zhang Yanping. The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID-19) — China, 2020. (2020) Available online at: http://weekly.chinacdc.cn/en/article/id/e53946e2-c6c4-41e9-9a9bfea8db1a8f51 (accessed February 18, 2020).
56. Petersen R, Pan L, Blanck HM. Racial and ethnic disparities in adult obesity in the United States: CDC's tracking to inform state and local action. Prev Chronic Dis. (2019) 16:180579. doi: 10.5888/pcd16.180579
57. Wang L, Southerland J, Wang K, Bailey BA, Alamian A, Stevens MA, et al. Ethnic differences in risk factors for obesity among adults in California, the United States. (2017) 2017:2427483. doi: 10.1155/2017/2427483
58. Covid-19 Causes Sudden Strokes in Young Adults Doctors Say - CNN. Available online at: https://edition.cnn.com/2020/04/22/health/strokes-coronavirus-young-adults/index.html (accessed April 24, 2020).
59. Wang J, Hajizadeh N, Moore EE, McIntyre RC, Moore PK, Veress LA, et al. Tissue plasminogen activator (tPA) treatment for COVID-19 associated acute respiratory distress syndrome (ARDS): a case series. J Thromb Haemost . (2020) 1–4. doi: 10.1111/jth.14828
60. Lancet T, Medicine R. Comment Understanding pathways to death in patients with. Lancet Respir Med. (2020) 2019:2019–21. doi: 10.1016/S2213-2600(20)30165-X
61. Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA . (2020) 323:1775–6. doi: 10.1001/jama.2020.4683
62. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
63. Doctors Warn COVID-19 Might Cause Strokes in Young Adults. Available online at: https://nypost.com/2020/04/23/doctors-warn-covid-19-might-cause-strokes-in-young-adults/ (accessed April 24, 2020).
64. “Solidarity” Clinical Trial for COVID-19 Treatments. Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov/solidarity-clinical-trial-for-covid-19-treatments (accessed April 23, 2020).
65. Search, of: COVID-19 - List Results - ClinicalTrials.gov . Available online at: https://www.clinicaltrials.gov/ct2/results?cond=COVID-19&term=&cntry=&state=&city=&dist= (accessed May 1, 2020).
66. De Wilde AH, Jochmans D, Posthuma CC, Zevenhoven-Dobbe JC, Van Nieuwkoop S, Bestebroer TM, et al. Screening of an FDA-approved compound library identifies four small-molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture. Antimicrob Agents Chemother. (2014) 58:4875–84. doi: 10.1128/AAC.03011-14
67. Tai DYH. Pharmacologic treatment of SARS: current knowledge and recommendations. Ann Acad Med Singapore. (2007) 36:438–43.
PubMed Abstract | Google Scholar
68. Sheahan TP, Sims AC, Leist SR, Schäfer A, Won J, Brown AJ, et al. Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV. Nat Commun. (2020) 11:222. doi: 10.1038/s41467-019-13940-6
69. Gao J, Tian Z, Yang X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci Trends. (2020) 14:72–73. doi: 10.5582/bst.2020.01047
70. Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. (2020) 30:269–71. doi: 10.1038/s41422-020-0282-0
71. Vincent MJ, Bergeron E, Benjannet S, Erickson BR, Rollin PE, Ksiazek TG, et al. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virol J. (2005) 2:1–0. doi: 10.1186/1743-422X-2-69
72. Cramer CL, Patterson A, Alchakaki A, Soubani AO. Immunomodulatory indications of azithromycin in respiratory disease: a concise review for the clinician. Postgrad Med. (2017) 129:493–9. doi: 10.1080/00325481.2017.1285677
73. Plaquenil™ Hydroxychloroquine Sulfate Tablets USP Description. Available online at: http://www.cdc.gov/malaria (accessed April 21, 2020).
74. Magagnoli J, Narendran S, Pereira F, Cummings T, Hardin JW, Sutton SS, et al. Outcomes of hydroxychloroquine usage in United States veterans hospitalized with Covid-19. medRxiv. (2020) doi: 10.1101/2020.04.16.20065920
75. Shamshirian A, Hessami A, Heydari K, Alizadeh-Navaei R, Ebrahimzadeh MA, Ghasemian R, et al. Hydroxychloroquine Versus COVID-19: A Rapid Systematic Review and Meta-Analysis. medRxiv. (2020) doi: 10.1101/2020.04.14.20065276
76. Li G, De Clercq E. Therapeutic options for the 2019 novel coronavirus (2019-nCoV). Nat Rev Drug Discov . (2020) 19:149–50. doi: 10.1038/d41573-020-00016-0
77. Warren TK, Jordan R, Lo MK, Ray AS, Mackman RL, Soloveva V, et al. Therapeutic efficacy of the small molecule GS-5734 against Ebola virus in rhesus monkeys. Nature. (2016) 531:381–5. doi: 10.1038/nature17180
78. Williamson BN, Feldmann F, Schwarz B, Meade-White K, Porter DP, Schulz J, et al. Clinical benefit of remdesivir in rhesus macaques infected with SARS-CoV-2. bioRxiv. (2020) doi: 10.1101/2020.04.15.043166
79. Wang Y, Zhang D, Du G, Du R, Zhao J, Jin Y, et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. (2020) 395:1569–78. doi: 10.1016/S0140-6736(20)31022-9
80. Cao B, Wang Y, Wen D, Liu W, Wang J, Fan G, et al. A trial of lopinavir–ritonavir in adults hospitalized with severe covid-19. N Engl J Med . (2020) 382:1787–99. doi: 10.1056/NEJMoa2001282
81. Search, of: Lopinavir, Ritonavir, | COVID - List Results - ClinicalTrials.gov . Available online at: https://clinicaltrials.gov/ct2/results?term=Lopinavir%2CRitonavir&cond=COVID&draw=4&rank=22#rowId21 (accessed April 23, 2020).
82. Bhatnagar T, Murhekar M, Soneja M, Gupta N, Giri S, Wig N, et al. Lopinavir/ritonavir combination therapy amongst symptomatic coronavirus disease 2019 patients in India: protocol for restricted public health emergency use. Indian J Med Res. (2020) 151:184–9. doi: 10.4103/ijmr.IJMR_502_20
83. Yeh K-M, Chiueh T-S, Siu LK, Lin J-C, Chan PKS, Peng M-Y, et al. Experience of using convalescent plasma for severe acute respiratory syndrome among healthcare workers in a Taiwan hospital. J Antimicrob Chemother. (2005) 56:919–22. doi: 10.1093/jac/dki346
84. Shen C, Wang Z, Zhao F, Yang Y, Li J, Yuan J, et al. Treatment of 5 critically Ill patients with COVID-19 with convalescent plasma. JAMA . (2020) 323:1582–9. doi: 10.1001/jama.2020.4783
85. Cao W, Liu X, Bai T, Fan H, Hong K, Song H, et al. High-dose intravenous immunoglobulin as a therapeutic option for deteriorating patients with coronavirus disease 2019. Open Forum Infect Dis . (2020) 7:1–6. doi: 10.1093/ofid/ofaa102
86. Bloch EM, Shoham S, Casadevall A, Sachais BS, Shaz B, Winters JL, et al. Deployment of convalescent plasma for the prevention and treatment of COVID-19. J Clin Invest . (2020) 138745:1–22. doi: 10.1172/JCI138745
87. Ye M, Fu D, Ren Y, Wang F, Wang D, Zhang F, et al. Treatment with convalescent plasma for COVID-19 patients in Wuhan, China. J Med Virol. (2 020) doi: 10.1002/jmv.25882
88. Recommendations for Investigational COVID-19 Convalescent Plasma | FDA. Available online at: https://www.fda.gov/vaccines-blood-biologics/investigational-new-drug-ind-or-device-exemption-ide-process-cber/recommendations-investigational-covid-19-convalescent-plasma (accessed April 23, 2020).
89. Search, of: plasma | Interventional Studies | COVID - List Results - ClinicalTrials.gov . Available online at: https://clinicaltrials.gov/ct2/results?term=plasma&cond=COVID&Search=Apply&age_v=&gndr=&type=Intr&rslt= (accessed April 23, 2020).
90. Infection Prevention and Control. Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/infection-prevention-and-control (accessed February 17, 2020).
91. Wilder-Smith A, Freedman DO. Isolation, quarantine, social distancing and community containment: pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J Travel Med . (2020) 27:taaa020. doi: 10.1093/jtm/taaa020
92. Press Information Bureau AYUSH Advisory for Corona virus. Press Inf Bereau. Available online at: https://pib.gov.in/PressReleasePage.aspx?PRID=1600895 (accessed February 17, 2020).
93. CanSino, Biologics : China Announces First Human Trials of Covid-19 Vaccine | MarketScreener,. Available online at: https://www.marketscreener.com/CANSINO-BIOLOGICS-INC-59318312/news/CanSino-Biologics-China-announces-first-human-trials-of-Covid-19-vaccine-30183232/ (accessed April 7, 2020).
94. Safety, and Immunogenicity Study of 2019-nCoV Vaccine (mRNA-1273) for Prophylaxis SARS CoV-2 Infection - Full Text View - ClinicalTrials.gov . Available online at: https://clinicaltrials.gov/ct2/show/NCT04283461 (accessed April 7, 2020).
95. NIH, Clinical Trial of Investigational Vaccine for COVID-19 Begins | National Institutes of Health (NIH),. Available at: https://www.nih.gov/news-events/news-releases/nih-clinical-trial-investigational-vaccine-covid-19-begins (accessed April 7, 2020).
96. Novel, Coronavirus vaccine manufacturing contract signed — The Jenner Institute,. Available online at: https://www.jenner.ac.uk/about/news/novel-coronavirus-vaccine-manufacturing-contract-signed (accessed April 7, 2020).
97. Xie L, Sun C, Luo C, Zhang Y, Zhang J, Yang J, et al. SARS-CoV-2 and SARS-CoV Spike-RBD structure and receptor binding comparison and potential implications on neutralizing antibody and vaccine development. bioRxiv [Preprint]. (2020). doi: 10.1101/2020.02.16.951723
98. The Global Economic Impact of the Coronavirus Outbreak – Harvard Gazette. Available online at: https://news.harvard.edu/gazette/story/2020/02/the-global-economic-impact-of-the-coronavirus-outbreak/ (accessed February 17, 2020).
99. Shimizu K. 2019-nCoV, fake news, and racism. Lancet . (2020) 395:685–6. doi: 10.1016/S0140-6736(20)30357-3
100. ROHDE RODNEY. 2019 Novel Coronavirus (2019-nCoV) Update: Uncoating the Virus. Am Soc Microbiol. (2020). Available online at: https://asm.org/Articles/2020/January/2019-Novel-Coronavirus-2019-nCoV-Update-Uncoating
101. Virus-free Indonesia more threatened by COVID-19 than Singapore Malaysia: Survey - World - The Jakarta Post. Available online at: https://www.thejakartapost.com/news/2020/02/18/virus-free-indonesia-more-threatened-by-covid-19-than-singapore-malaysia-survey.html (accessed February 18, 2020).
102. Japan, May Lose $1,.29 Billion in Tourism Revenue Due to COVID-19 Outbreak | The Japan Times. Available online at: https://www.japantimes.co.jp/news/2020/02/16/business/economy-business/japan-lose-billion-tourism-revenue-covid19-outbreak/#.XkvxX0fitPY (accessed February 18, 2020).
103. Coronavirus's Effect on Tourism Will Carry Into 2021 Experts Say - Bloomberg. Available online at: https://www.bloomberg.com/news/articles/2020-02-13/coronavirus-s-effect-on-tourism-will-carry-into-2021-experts-say (accessed February 18, 2020).
104. The, week in charts - The cost of covid-19 | Graphic detail | The Economist,. Available online at: https://www.economist.com/graphic-detail/2020/02/14/the-cost-of-covid-19 (accessed February 17, 2020).
105. coronavirus: Covid-19 Impact: Pharma Companies Feel the Pain as Prices of Key Inputs Shoot Up - The Economic Times. Available online at: https://economictimes.indiatimes.com/industry/healthcare/biotech/pharmaceuticals/covid-19-impact-pharma-companies-feel-the-pain-as-prices-of-key-inputs-shoot-up/articleshow/74144044.cms?from=mdr (accessed February 17, 2020).
106. Coronavirus Outbreak: Paracetamol Prices Jump 40% In India As Coronavirus Shuts Down China. Available online at: https://www.ndtv.com/india-news/coronavirus-outbreak-paracetamol-prices-jump-40-in-india-as-coronavirus-shuts-down-china-2181480 (accessed February 18, 2020).
107. The coronavirus could cripple China's economy for longer than Wall Street wants to believe | Business Insider India. Available online at: https://www.businessinsider.in/international/news/the-coronavirus-could-cripple-chinas-economy-for-longer-than-wall-street-wants-to-believe/articleshow/74162183.cms (accessed February 17, 2020).
108. Viral Slowdown - How China's Coronavirus Epidemic Could Hurt the World Economy | Leaders | The Economist. Available online at: https://www.economist.com/leaders/2020/02/13/how-chinas-coronavirus-epidemic-could-hurt-the-world-economy (accessed February 17, 2020).
109. China's Economic Battle With COVID-19 | The ASEAN Post. Available online at: https://theaseanpost.com/article/chinas-economic-battle-covid-19 (accessed February 17, 2020).
110. The Coronavirus Could Cost China's Economy $60 Billion this Quarter. - CNN. Available online at: https://edition.cnn.com/2020/01/31/economy/china-economy-coronavirus/index.html (accessed February 18, 2020).
Keywords: 2019-nCoV, COVID-19, SARS-CoV-2, coronavirus, pandemic, SARS
Citation: Keni R, Alexander A, Nayak PG, Mudgal J and Nandakumar K (2020) COVID-19: Emergence, Spread, Possible Treatments, and Global Burden. Front. Public Health 8:216. doi: 10.3389/fpubh.2020.00216
Received: 21 February 2020; Accepted: 11 May 2020; Published: 28 May 2020.
Reviewed by:
Copyright © 2020 Keni, Alexander, Nayak, Mudgal and Nandakumar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY) . The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Krishnadas Nandakumar, mailnandakumar77@gmail.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Lessons from pandemics: Due to panic-buying, consumers bought things they didn't need
A new study by concordia university in canada found that consumers largely panic-bought during the covid-19 pandemic, and lessons that could be learned for future events..
 testing site in New York City, New York, U.S., December 12, 2022.")
What did the study find?
")
Important adjustments for our commencement celebrations: May 13, 2024
To the Case Western Reserve University community,
Commencement marks the culmination of years of hard work and dedication in classrooms, labs, clinicals, internships, extracurriculars and so much more. Though this always is one of our favorite events of any year, we are especially looking forward to this year’s festivities, as many members of the undergraduate Class of 2024 had their high school graduation ceremonies canceled at the start of the COVID-19 pandemic.
This is an exceptional time for our soon-to-be alumni and their families, and we are eager to celebrate alongside them. While we are aware some individuals may have plans to disrupt these events, we are committed to ensuring this day remains centered on our outstanding graduates and their achievements.
To that end, we want to share general guidelines and expectations for ensuring commencement and other end-of-semester events are safe, welcoming and civil environments for all.
First and foremost: As an institution of higher education, Case Western Reserve is committed to the critical importance of public discourse and freedom of expression. However, our freedom of expression policy also notes that the university “may reasonably regulate the time, place, and manner of expression to ensure that it does not disrupt the ordinary activities of the university.”
As noted Friday, all gatherings and events related to freedom of expression, regardless of perspective or subject, taking place between now and May 20 on university property will require reservations that are approved in writing by the interim vice president for student affairs (via [email protected] ) to ensure safety and adherence to policy. Participation in an unapproved activity on Case Western Reserve property—including protest during commencement—will result in referral to the relevant conduct process, even for those scheduled to graduate.
Our top priority is always the safety of our community, and actions or language—including decorations on mortar boards—that make others feel threatened or intimidated will not be tolerated. In addition, we are updating our security measures for Wednesday’s convocation events as well as all diploma ceremonies including:
- Metal detectors, bag screenings and visual inspection of clothing capable of concealing prohibited items upon entry to convocation and all diploma ceremonies (please note: graduates will need to remove mortar boards to proceed through metal detectors);
- A range of prohibite d items —including signage, banners and flags, and bags larger than 5”x8”x1”;
- Ticketing for convocation and all diploma ceremonies held in Veale Convocation, Recreation and Athletic Center and the Maltz Center for Performing Arts; and
- ID checks (CWRU ID or other photo identification, e.g., driver’s license) for all attendees at convocation events and for graduating students at all diploma ceremonies.
The university also has implemented an opt-in emergency messaging system for guests; if an incident occurs about which the university needs to send an alert, guests who opt in (by texting “CWRUGrad2024” to 67283) will receive the same emergency message as our students, faculty and staff.
University staff and faculty members also have been trained on how to minimize disruptions, if needed, and quickly restore the event’s focus to our graduates’ accomplishments.
We are committed to maintaining an environment that ensures our Class of 2024 can be honored with a celebration befitting their incredible achievements. We hope you’ll join us in recognizing them .
Sincerely, Eric W. Kaler President
Joy K. Ward Provost and Executive Vice President

Chiefs star gives controversial commencement speech
K ansas City Chiefs star kicker Harrison Butker served as the guest commencement speaker for Benedictine College in Kansas over the weekend, delivering a speech for the graduating class that was not shy on controversial opinions on heated topics.
From the COVID-19 pandemic to LGBTW Pride Month to President Joe Biden, Butker had plenty to say about all of the above. And his traditional Catholic values certainly shined through throughout the speech.
“You missed out on so many milestones that us older people have taken for granted,” said Butker referring to the COVID-19 pandemic. “While COVID may have played a large role throughout your formative years, it is not unique. Bad policies and poor leadership have negatively impacted major life issues. Things like abortion, IVF, surrogacy, euthanasia, as well as a growing support for degenerate cultural values in media all stem from the pervasiveness of disorder.
“Our own nation is led by a man who publically and proudly proclaims his Catholic faith. But at the same time is delusional enough to make the sign of the cross during a pro-abortion rally. He has been so vocal in his support for the murder of innocent babies that I’m sure to many people it appears that you can be both Catholic and pro-choice. He is not alone. From the fan behind the COVID lockdown, to the people pushing gender ideologies onto the youth of America. They all have a glaring thing in common. They are all Catholic.”
Later in the speech, he referred to LGBTQ Pride Month, which takes place in June, as a month that is dedicated to “deadly sin”.
“I’m certain the reporters at the AP could not have imagined that their attempt to rebuke and embarrass places and people like those here at Benedictine wouldn’t be met with anger, but instead met with excitement and pride,” Butker said. “Not the deadly sin sort of pride that has an entire month dedicated to it, but true God-centered pride that is cooperating with the Holy Ghost to glorify him.”
Butker certainly got all of his points across in the 20-minute speech on Saturday, which can be seen in its entirety on the Benedictine College YouTube page. But he certainly could face some backlash for a number of these highly debated opinions.
[ Benedictine College on YouTube ]
The post Chiefs star gives controversial commencement speech appeared first on Next Impulse Sports .

Click through the PLOS taxonomy to find articles in your field.
For more information about PLOS Subject Areas, click here .
Loading metrics
Open Access
Peer-reviewed
Research Article
Violence against women on Twitter in India: Testing a taxonomy for online misogyny and measuring its prevalence during COVID-19
Roles Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing
* E-mail: [email protected]
Affiliation UNICEF, UNICEF HQ, New York, New York, United States of America
Roles Methodology, Supervision, Writing – review & editing
Affiliation Department of Computer Science, School of Engineering, University of California San Diego, San Diego, California, United States of America
Affiliation Center on Gender Equity and Health, Department of Medicine, University of California San Diego, San Diego, California, United States of America
Roles Supervision, Writing – review & editing
Affiliation Division of Health Promotion and Behavioral Science, School of Public Health, San Diego State University, San Diego, California, United States of America
Affiliation School of Social Work, San Diego State University, San Diego, California, United States of America
Roles Funding acquisition, Methodology, Supervision, Writing – review & editing
- Nabamallika Dehingia,
- Julian McAuley,
- Lotus McDougal,
- Elizabeth Reed,
- Jay G. Silverman,
- Lianne Urada,
- Published: October 25, 2023
- https://doi.org/10.1371/journal.pone.0292121
- Peer Review
- Reader Comments
Online misogyny is a violation of women’s digital rights. Empirical studies on this topic are however lacking, particularly in low- and middle- income countries. The current study aimed to estimate whether prevalence of online misogyny on Twitter in India changed since the pandemic.
Based on prior theoretical work, we defined online misogyny as consisting of six overlapping forms: sexist abuses, sexual objectification, threatening to physically or sexually harm women, asserting women’s inferiority, justifying violence against women, and dismissing feminist efforts. Qualitative analysis of a small subset of tweets posted from India (40,672 tweets) substantiated this definition and taxonomy for online misogyny. Supervised machine learning models were used to predict the status of misogyny across a corpus of 30 million tweets posted from India between 2018 and 2021. Next, interrupted time series analysis examined changes in online misogyny prevalence, before and during COVID-19.
Qualitative assessment showed that online misogyny in India existed most in the form of sexual objectification and sexist abusive content, which demeans women and shames them for their presumed sexual activity. Around 2% of overall tweets posted from India between 2018 and 2021 included some form of misogynistic content. The absolute volume as well as proportion of misogynistic tweets showed significant increasing trends after the onset of COVID-19, relative to trends prior to the pandemic.
Findings highlight increasing gender inequalities on Twitter since the pandemic. Aggressive and hateful tweets that target women attempt to reinforce traditional gender norms, especially those relating to idealized sexual behavior and framing of women as sexual beings. There is an urgent need for future research and development of interventions to make digital spaces gender equitable and welcoming to women.
Citation: Dehingia N, McAuley J, McDougal L, Reed E, Silverman JG, Urada L, et al. (2023) Violence against women on Twitter in India: Testing a taxonomy for online misogyny and measuring its prevalence during COVID-19. PLoS ONE 18(10): e0292121. https://doi.org/10.1371/journal.pone.0292121
Editor: Mahdi Zareei, Technologico de Monterrey, MEXICO
Received: November 8, 2022; Accepted: September 13, 2023; Published: October 25, 2023
Copyright: © 2023 Dehingia et al. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: All relevant data necessary for replicating the study findings can be found here: https://doi.org/10.7910/DVN/H3IXDN .
Funding: This study was funded by the Bill and Melinda Gates Foundation Grant No. OPP1163682. The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Competing interests: The authors have declared that no competing interests exist.
Introduction
Violence against women (VAW) on online platforms is a violation of women’s digital rights. It can push women out of online spaces, and impact their social, economic, as well as health outcomes [ 1 ]. One of the most prevalent forms of online VAW, online misogyny or hate speech against women refers to any content that tries to threaten, intimidate, and shame women, or any rhetoric that emphasizes the authority of men over women [ 1 ]. According to a multi-country online survey in 2019, around two-thirds of women users of the internet reported having received some form of sexist or hateful language designed to attack or humiliate them [ 2 ]. Such experiences can often cause increased anxiety, depression, and lower self-esteem among women [ 3 , 4 ]. The extent and frequency of misogynistic attacks varies across different groups of women; younger women, and women belonging to marginalized racial or sexual identity groups are more at risk of experiencing online misogyny [ 2 , 5 – 9 ]. The past two years have thus noted an increasing number of calls, for hate speech regulation on social media platforms [ 10 , 11 ].
The majority of the existing research on online violence, including online misogyny, has focused on high-income countries, primarily due to greater digital access and use of social media platforms in these regions [ 12 ]. To our knowledge, no academic study has examined the characteristics of online misogyny in low- and middle-income countries (LMIC). This presents a key gap in literature, given that the use of social media, and consequently, the amount of online hateful content, has increased rapidly in LMICs in recent years [ 13 , 14 ]. India, in particular, is an important geography to examine online misogyny. Compared to many other LMICs, adverse gender norms and offline forms of gender-based violence are more prevalent in the country [ 15 , 16 ], putting women at a higher risk of experiencing violence in online spaces. Use of social media platforms is also on the rise in the country. As of January 2022, India had over 25 million active Twitter users, with a 30% increase in average daily users in 2020. Although Twitter has an urban bias; most Twitter users in the country are likely to be educated, living in cities, and of middle to high wealth status [ 17 ]. Nonetheless, Twitter is being frequently used as a key platform for feminist discussions and organizing in India [ 18 ], which can increase the likelihood of misogynist expression as a backlash [ 19 ]. The current study aims to contribute to the growing literature on online VAW on social media platforms, by measuring online misogyny on Twitter in India.
Limited global research suggests a potential increase in this form of violence since the pandemic, impacting millions of women daily [ 10 ]. An analysis of tweets and Facebook posts from South and South-east Asia by United Nations Women found 168 percent increase in misogynistic content during March-June 2020, when compared to the same period in 2019 [ 20 ]. However, despite many such analyses of the effect of COVID-19 on online content, little is known about the features and prevalence of online misogyny, and how it might have changed over the course of the pandemic. In this study, we take a first step to provide temporal estimates of online misogyny on Twitter in India from 2018 to 2021, and systematically examine any changes in its rates of increase/decrease before and during COVID-19.
As early as May 2020, the United Nations Secretary General made a global appeal to tackle COVID-19 influenced hate speech on digital platforms, with hateful content covering “ stereotyping , stigmatization , and the use of derogatory , misogynistic , racist , xenophobic , Islamophobic or antisemitic language ” [ 21 ]. Potential drivers of such hate speech during the pandemic include increased isolation due to stay-at-home orders, greater use of social media platforms, greater exposure to polarizing and differing views on the social media platforms, and fear, uncertainty, and anxiety of living through the pandemic [ 22 ]. Isolation is a strong motivational factor for hate speech on social media [ 23 ], and the confined living conditions, health and financial worries following the lockdown can create tension and stress, increasing the risk for online expression of hate speech. With regards to hate speech against women in particular, global evidence in support of increasing cases of gender-based violence during the pandemic further points to a potential increase in violence against women on online platforms [ 24 ]. An analysis of Twitter data before and after the onset of COVID-19 will allow us to test this hypothesis of increased levels of misogyny on Twitter since the pandemic.
Defining online misogyny
A key reason for the limited empirical evidence on online misogyny, is the lack of a standard taxonomy [ 25 ]. A majority of existing research on this topic has lacked theoretical considerations, classifying it as content that includes identifiable sexist slurs [ 26 – 28 ]. Earlier works on misogyny detection relied on lexicon-based methods, where misogynistic tweets were identified based on the presence of gendered abusive words [ 29 , 30 ]. Anzovino et. al (2018) introduced a benchmark dataset of tweets classified as misogynistic, with online misogyny defined as consisting of five forms: a) slurring, b) stereotypes, c) sexual harassment and threats, d) dominance to preserve men’s control, and e) derailing to justify VAW [ 31 , 32 ]. Multiple other studies have used this definition for misogyny detection [ 33 , 34 ]. We build on this taxonomy, by adapting it to the context of India, and locating it within a theoretical understanding of misogyny as a notion central to the feminist theory.
Feminist theory posits that misogyny, whether online or offline, stems from patriarchal values justifying men’s control over women via degradation and violence; misogyny actively seeks to silence women and maintain the status quo of patriarchal gender roles [ 35 ]. Sobieraj describes intimidating, shaming, and discrediting as the three key strategies often adopted by perpetrators of online misogyny, where attackers draw on women’s fear of sexual assault and physical violence to intimidate them, sexually objectify to publicly shame them, and discredit or dismiss their achievements as well as their fight to equality [ 1 ]. Asserting the inferiority of women, dismissing feminist movements, and objectifying women or viewing women primarily as an object of men’s desire, are thus at the heart of misogyny [ 36 ]. Our preliminary research on misogyny detection in South-Asian countries noted an emphasis on dismissal of feminist thought and discrediting of women’s claims of gender-based violence [ 37 ]. Guided by these theoretical and empirical works, we define online misogyny as any rhetoric or content that uses hostile and malicious language targeted at women, objectifies them, threatens them with physical or sexual harm, tries to assert their inferiority, justifies gender-based violence, or discredits feminist activists and their efforts. By qualitatively analyzing a large dataset of tweets (over 40,000 tweets), we first test whether this definition and taxonomy is valid for content posted on Twitter from India. This is followed by estimation of temporal online misogyny, using machine learning techniques that rely on the validated taxonomy. Our study objectives are two-fold: a) testing a taxonomy for online misogyny in India that is rooted in feminist theory, and b) using this taxonomy, estimate whether prevalence of online misogyny on Indian Twitter changed since the pandemic, across a sample of 30 million tweets posted between 2018 and 2021. Given the current lack of research on the extent and forms of misogyny on Twitter in LMICs, our study hopes to generate evidence that can be used to advocate for policies and strategies to address misogyny on Twitter.
Online misogyny taxonomy
We define online misogyny as consisting of six broad and overlapping forms: a) sexist abusive content, b) sexual objectification, c) threatening to physically or sexually harm women (presence of sexist language that indicates the threat being directed at women), d) asserting inferiority, e) justifying VAW, and f) dismissing feminist efforts. We provide definitions and example tweets for each form of online misogyny as Supporting Information. This taxonomy is guided by feminist theoretical work on misogyny [ 36 ], prior research on online misogyny detection, particularly the studies by Anzovino et. al (2018) , and our preliminary research on measuring online misogyny in South Asian countries.
Extracting geolocated tweets
We used geotagged English language tweets posted from India between January 2018 and December 2021 (30 million tweets). All tweets were extracted using the official Twitter API for academic research, which allows extraction of historical tweets. The most recent 800–1000 tweets published every hour from January 1 st 00:00 2018 to December 31 st 23:00 2021 were collected.
We used supervised machine learning models to classify tweets as misogynist/non-misogynist, as well as the six different forms of misogyny. Fig 1 depicts the different steps involved in our analysis. We describe each step in detail in the following sections.
- PPT PowerPoint slide
- PNG larger image
- TIFF original image
https://doi.org/10.1371/journal.pone.0292121.g001
Qualitative analysis of tweets for misogyny
Supervised machine learning models require a ground truth dataset. To that end, two trained undergraduate students first qualitatively coded a small subset of tweets, as misogynist/non-misogynist, and the six forms of misogyny. The selection of the subset of tweets was done using two approaches. First, from the large corpus of geotagged tweets between 2018 and 2020, we extracted posts containing representative keywords frequently used to harass and abuse women. To identify keywords, we contacted authors of an academic study on hate speech detection on Twitter. They used a list of keywords for different types of hate speech on Twitter, including misogyny [ 38 ]. We added a few words relevant to the Indian context to this list. Identified words included abusive terms, as well as generic words related to gender such as " woman ", " feminism " etc. It is key to note here that there may be certain tweets that contain abusive words, but might be non-offensive in their use and overall meaning. The inclusion of all such tweets that contained abusive words allowed us to build a ground truth dataset that identified the nuances in the use of abusive words. With this process, we selected a subset of 35,672 tweets.
Next, we chose a random subset of 5,000 tweets from the large corpus of geotagged tweets from 2018–2020. This dataset was included to ensure that tweets unrelated to women or gender were also represented in our ground truth sample. The main goal of using the two separate approaches to build the ground truth dataset was to collect a set of tweets that would have an adequate representation of both misogynist and non-misogynist tweets. A total of 40,672 tweets were thus selected for qualitative coding, with these two processes.
The qualitative coding of the tweets was carried out in two phases. First, the subset of tweets was coded as misogynist or non-misogynist by five trained undergraduate students. Every tweet was classified by at least two coders. Inter-rater kappa scores were calculated to examine reliability of the coding [ 39 ]. Any disagreement between the coders was resolved by the lead author of the study. Next, all tweets classified as misogynist were coded by two graduate students experienced in gender research, as the six forms of online misogyny. Inter-rater kappa scores were calculated for this step as well. The qualitative coding of misogynist tweets provided us with the opportunity to validate our taxonomy of misogyny. The two researchers did not identify any content that was outside the purview of the six predefined categories.
Selection of features or independent variables
Tweets were cleaned before running any machine learning model. This included deleting urls and ignoring punctuation and case. We also removed stop words, which are commonly used words such as “is”, “the”, “a” etc., from our text data. The decision to drop stop words was made after running multiple models with and without stop words. Next, the data was processed with text vectorization , in order for the machine learning regression models to mathematically interpret it. Text vectorization refers to the process of creating features or input variables in a model (independent variables in public health terminology). There are multiple methods for generating features or independent variables from text data. We used three types of feature selection methods: a) term frequency-inverse document frequency (TF-IDF) unigrams, b) TF-IDF unigrams and bigrams, and c) TF-IDF unigrams, bigrams, and linguistic features (number of words and number of adjectives). These methods were chosen based on guidelines suggested by a previous study on abuse detection [ 32 ]. TF-IDF is weighted word frequency, and reflects how important a word is to a document in a collection or corpus [ 40 ]. While TF-IDF with unigrams concerns with single words only, TF-IDF with unigrams and bigrams includes sequences of two words along with singular words. In addition to weighted word frequencies, linguistic features such as length of the tweet or number of adjectives in a tweet can also provide meaningful information about the content of the tweet. It is possible that tweets that are misogynist are shorter in length and have a relatively higher number of adjectives (abusive words or sentiments).
Running supervised machine learning models and predicting misogyny: Train and test models for best fit
We randomly split our data into a train and test dataset in a 70:30 ratio. The training dataset is used to train the machine learning model, while the test dataset is used to assess the performance of the trained model. To estimate the hyperparameters to be specified in the training model, we used a k-fold validation process. In this method, the training data are partitioned into k subsets of approximately equal size and one of the subsets becomes the validation set where the hyperparameters are validated. The remaining k-1 subsets are used as training data and this process is repeated.
We ran five different types of supervised machine learning models to classify tweets as misogynist/non-misogynist: a) Naïve Bayes (NB), b) Support Vector Machine (SVM), c) Ridge logistic regression, d) Multi-layer Perceptron Neural Network (MPNN), and e) Bidirectional Encoder Representations from Transformers (BERT). Naïve Bayes is a probabilistic model based on Bayes theorem and considers a strong independence assumption [ 41 ]. SVMs are based on a structural risk minimization principle, which aims to test a hypothesis for which we can guarantee the lowest true error. SVMs aim to create a hyperplane ( maximum-marginal hyperplane ), which separates the categories of the outcome label [ 42 ]. MPNN are complex non-linear models with a hierarchical or multi-layered structure. These models have been commonly used in text classification tasks [ 32 ]. BERT is a pre-trained language model (BERT is pretrained on a large corpus of English texts from Wikipedia and BookCorpus), with transformer architecture [ 43 ]. Transformers learn contextual relations between words; they are deep learning models where each output element is connected to every input element and the weightings between them are dynamically calculated. While previous models examine text sequences in a single direction (left-to-right or right-to-left training), BERT’s key difference and innovation is the application of bidirectional training. The BERT Transformer encoder reads the entire sequence of words at once. Specifically, we used the bert-large-uncased version, which consists of 24 layers (1024 hidden dimensions), 16 attention heads, and a total of 340M parameters. The Transformers library in Python was used to implement this approach.
The performance of each model was evaluated on the test set, by comparing actual labels or outcome variable values with the values predicted by the trained model. We used two evaluation metrics: (a) F1 score and (b) receiver operating characteristic—area under the curve (AUC). The receiver operating characteristic captures precision and recall at all potential decision thresholds, so the area under it is an appropriate metric to measure overall model performance. F1 score is the harmonic mean of precision and recall. The models with the best F1 and AUC estimates were chosen to predict the labels/outcome variable values for each tweet in our original dataset of over 30 million geotagged tweets posted between January 2018 to December 2021.
The analysis was repeated with each of the six forms of online misogyny as the outcome variable or label, with the sub-sample of tweets that was classified misogynist (N = 3894).
Analysis of misogyny prevalence pre and during COVID-19
Y t is the proportion of online misogyny related tweets, T is the time since COVID-19 related lockdown has been implemented in India (in days), X t is the dummy variable representing the imposition of lockdown, and X t T is an interaction term. β 1 represents the underlying pre-COVID-19 trend in misogyny prevalence, or the change in misogynistic tweets for every one unit time increase. β 2 captures the immediate effect of the onset of COVID-19, and β 3 represents the slope change in the proportion of misogynistic tweets following COVID-19, in comparison to trends prior to COVID-19. We ran interrupted time series regression models with two separate outcomes: a) total number of misogynistic tweets and b) proportion of misogynistic tweets per 100000 tweets.
Qualitative assessment of misogyny across tweets
Around 8% of the tweets that were qualitatively analyzed were classified as misogynist (N = 40,672). Among those identified as misogynist, 57% were related to sexual objectification, 34% covered sexist abusive content, 6% justified violence against women, and 5% were content that dismissed feminism or feminist efforts. A small proportion of misogynist tweets included threats of harm (1%) and assertion of authority (1%). The two researchers who conducted the qualitative coding did not identify any content that was outside the purview of the six predefined categories of online misogyny. The coding had good reliability, with an inter-rater kappa score of 0.87.
The tweets classified as sexual objectification (57%) included text that sexualized women’s body, shamed women for presumed sexual activity ( slut shaming ), and text that included lewd remarks and sexual solicitation. These tweets emphasized the treatment of women as sexual objects of men’s sexual desire. The category “justify violence against women” (6%) included tweets that highlighted the prevalence of rape myth acceptance and victim blaming among Twitter users. Tweets aggressively asserted that women needed to act a certain way to reduce the risk of rape and violence (e.g., not wear short clothes, not go out at night). This category also included tweets that aimed to derail the conversation from VAW, by focusing on “fake rape cases” in India. Around 10% of these tweets included the hashtag “#mentoo”, with tweets noting men’s victimization with fake rape allegations. Additionally, there were a small number of tweets (n = 3) that dismissed marital rape. For example, a tweet stated that all married women were free to be raped by their husbands.
The category on dismissal of feminist efforts included a number of tweets declaring feminism as a “virus”, with 13% of the tweets including the word “feminazis”. Around 16% of the tweets classified as dismissal of feminist efforts were also categorized as justifying VAW.
Machine learning models to predict misogyny
We ran the different types of machine learning models, separately for each outcome variable: misogyny, sexual objectification, sexist abusive content, justifying VAW, dismissing feminist efforts, threatening to harm, and asserting authority. For the analysis with misogyny as the outcome variable, BERT performed the best [ Table 1 ]. This was followed by the logistic regression models (with TF-IDF unigrams). The Naïve Bayes had the lowest values of AUC as well as F1 score, for misogyny prediction.
https://doi.org/10.1371/journal.pone.0292121.t001
Predicting online misogyny across tweets from 2018–2021 and examining prevalence
We used the specifications from our best performing model to predict misogyny across the large Twitter dataset of 30 million tweets. Each tweet in this dataset was classified as misogyny or non-misogyny by this model. Overall, 1.6% of the geotagged tweets collected from India included misogynist content.
We ran separate interrupted time series models with total number of misogynistic tweets, and proportion of misogynistic tweets per 100000 tweets as the outcomes ( Table 2 ). The volume of misogynistic tweets increased significantly by 30 times immediately after the onset of COVID-19, with increasing trends in the following months between April 2020-December 2021. The proportion of misogynistic tweets per 100000 tweets also showed significant and sustained increasing trends after the onset of COVID-19, relative to trends prior to the pandemic. However, there was a significant decrease immediately after the onset of COVID-19, followed by the increasing trends.
https://doi.org/10.1371/journal.pone.0292121.t002
Digital social media portals are often signaled to be democratic public spaces. However, we find that similar to the offline world, they are home to increasing gender inequalities. Our study observes online misogyny on Twitter in India to be prevalent, with increasing trends since COVID-19. Around 2% of overall daily tweets between 2018 and 2021 included some form of misogynistic content. This translates to millions of misogynistic tweets every day, given that around 20 billion tweets are posted daily on average. Our study draws attention to online misogyny as a topic for gender research in India, a country where internet use is on the rise and offline forms of gender-based violence are highly prevalent.
We find evidence in support of increasing trends in overall volume as well as proportion of misogynistic content on Twitter since the pandemic. However, our results show an immediate drop in the proportion of misogynistic tweets after the pandemic, followed by sustained and significant growth in the next two years. This could be because of an increase in tweets related to other relevant topics such as COVID-19, health services, and vaccines, right after the onset of the pandemic. Nonetheless, the sustained increasing trend after the initial drop is worrisome, and warrants further assessments of long-term changes. Our study contributes to the existing literature that shows significant increases in other offline forms of VAW since the pandemic.
We find that online misogyny exists in the form of sexual objectification, sexist abusive content, content that threatens to harm, asserts authority, justifies VAW, and dismisses feminism, with sexual objectification and sexual abuse of women being the most common forms. Multiple prior studies have shown online sexual harassment and victimization to be associated with adverse mental and psychological consequences, particularly for young girls [ 44 , 45 ]. Online sexual harassment is unique compared to offline experiences in that individuals who are not directly attacked by the abusers/social media users, are also exposed to the sexually charged posts. In addition to causing mental distress, for young users of the Internet, exposure to such content might cause endorsements of patriarchal beliefs that view women as sexual beings and normalize VAW, leading to a continuation of the cycle of violence [ 46 , 47 ]. While findings are related to the online world, this is indicative of an ongoing acceptability of sexual harassment in the country [ 48 ]. We find that sexual objectification related tweets also include content that shame women for their real or presumed sexual activity. Our findings show that online abusers often use women’s sexual autonomy as a weapon for demeaning and disrespecting them, further perpetuating adverse gender norms that deny women sexual freedom.
Another manifestation of online misogyny is the dismissal of feminist efforts, and justification of VAW. Resistance to advancement of gender equality is a common feature of the feminist struggle, and like the offline world, it is evidently present in the Indian Twitter space. This ‘backlash’ effect has been documented for offline movements, and it can take different forms such as denial of the issue, derailing of conversation, rejection of men’s responsibility, and discrediting of feminist activities [ 49 ]. Prior research has highlighted the disproportionate amount of online misogyny and violence directed at women politicians, journalists, and women engaging in feminist debate on Twitter. Our analysis did not classify tweets that were directed at specific women, but we found many posts that included words such as “ feminazis ”, and dismissed feminism as a “ problem ” and a “ virus ”. It is likely that such posts were directed at individuals who engage in conversations related to feminism or gender equality. Denial of the problem by focusing on fake rape allegations was another common theme across tweets categorized as justification of VAW. Such content, in addition to spreading disinformation, has the potential to widen digital gender inequalities by acting as triggering content for survivors of gender-based violence.
Currently, there are no dedicated legislations in India against gender-based cyber violence [ 50 ]. The laws protecting citizens from cyber hate do not specifically recognize sexist or misogynistic trolling. Our findings show that along with strengthening of laws and regulations to prevent online misogyny, shifting entrenched gender norms will be critical to achieving gender equality in digital spaces. Norms-based interventions addressing gender-based violence in general can consider inclusion of elements of digital violence in their programs.
In addition to providing insights on the prevalence and characteristics of online misogyny, our work is one of the first attempts to detect misogyny across a very large dataset of tweets from India. We tested multiple machine learning models, and found the pre-trained language model, BERT, to be the best performing models. However, our analysis is limited to English tweets only, and does not cover tweets in any Indian vernacular language. Future studies should consider building multilingual models to provide improved insights related to misogyny on Twitter in India.
Our study has a few additional limitations. First, our findings are likely to have an urban bias, representative of the English-speaking population, since our data was limited to English tweets only. Next, this study only includes geotagged tweets from India, which constitutes around 2% of the overall tweets. However, few prior studies have noted that the large number of tweets created daily ensure the adequateness of geotagged tweets in being a good representation of overall Twitter conversations [ 51 , 52 ]. Third, we examine the changes in prevalence of misogyny before and after the start of the pandemic. We do not take into account other relevant key events that might trigger changes in the amount of misogynistic expression. Finally, our study focusses solely on the misogyny directed against women in India, and does not cover transmisogyny or different intersectional categories as relates to race, ethnicity, age, and sexual orientation. Future research should consider including these aspects, given that younger individuals, and individuals belonging to minority groups are more likely to experience violence online [ 5 ].
Conclusions
The past couple of years have noted increasing activism against the growing levels of misogyny on Twitter as well as other social media platforms. Our findings emphasize the need for inclusion of digital violence in the broader policy discourse on gender-based violence; online misogyny is a continuum of violence experienced by women in their offline worlds in India. Aggressive and hateful tweets that target women in the country attempt to reinforce traditional gender norms, especially those relating to idealized sexual behavior and framing of women as sexual beings. Our study provides evidence on increasing trends of misogyny on Indian Twitter, and emphasizes the utility of machine learning methods in examination of aspects related to VAW, which can support future research and development of interventions to make these digital spaces equitable and welcome for women.
Supporting information
S1 file. annotation guidelines/manual for undergraduate student coders..
https://doi.org/10.1371/journal.pone.0292121.s001
S2 File. Definition and example tweet for each category of online misogyny.
https://doi.org/10.1371/journal.pone.0292121.s002
Acknowledgments
We are grateful to Dr. James Fowler who supported us in accessing the Twitter data. We thank Riley Saham, Mairen Oates, Aviram Raj-Silverman, Lucas Fowler, and Max Goldberg, for serving as qualitative coders of the Twitter dataset. We are grateful to Wendy Wei Cheung for carrying out the qualitative coding of misogynist tweets.
- 1. Sobieraj S. Credible threat: Attacks against women online and the future of democracy: Oxford University Press; 2020.
- 2. The Economist Intelligence Unit (EIU). Measuring the prevalence of online violence against women New York: The Economist Intelligence Unit; 2020 [ https://onlineviolencewomen.eiu.com/ .
- 3. Amnesty International. Amnesty reveals alarming impact of online abuse against women: Amnesty International; 2017 [ https://www.amnesty.org/en/latest/news/2017/11/amnesty-reveals-alarming-impact-of-online-abuse-against-women/ .
- 4. Amnesty TT. A Toxic Place for Women, 2018.
- 5. deSHAME P. Young people’s experiences of online sexual harassment. ChildNet; 2017.
- View Article
- Google Scholar
- 7. Amnesty I. Toxic Twitter: a Toxic Place for Women. Report. 2018.
- 9. Pew Research Center. Pew Report on Online Harassment 2017. 2017.
- 10. UN Women. Online and ICT facilitated violence against women and girls during COVID-19. 2020.
- 11. Wang S, Affoum N. Cyber harassment: A growing concern in the age of COVID. In: World Bank, editor. 2021.
- 13. Jeremy Liebowitz, Geoffrey Macdonald, Vivek Shivaram, Vignaraja S. The Digitalization of Hate Speech in South and Southeast Asia: Conflict-Mitigation Approaches. Georgetown University of International Affairs2021.
- 14. Minority Rights. South Asia State of Minorities Report 2021 –Hate Speech against Minorities. South Asia Collective; 2022.
- 15. National Crime Records B. Crime in India 2016: Statistics. Ministry of Home Affairs, Government of India New Delhi; 2016.
- 16. IIPS & ICF. National Family Health Survey (NFHS-4) 2015–16. Mumbai, India; 2017.
- 17. Ananya Bhattacharya. In India, the internet is a place for cityfolk and men. Quartz India. 2018.
- 20. UN Women. ELIMINATING ONLINE HATE SPEECH TO SECURE WOMEN’S POLITICAL PARTICIPATION. 2021.
- 21. United Nations. United Nations Guidance Note on Addressing and Countering COVID-19 related Hate Speech. United Nations; 2020.
- PubMed/NCBI
- 23. Von Behr I. Radicalisation in the digital era: The use of the internet in 15 cases of terrorism and extremism. 2013.
- 27. National Democratic Institute. Tweets That Chill: Analyzing Online Violence Against Women in Politics. 2019.
- 30. Hewitt S, Tiropanis T, Bokhove C, editors. The problem of identifying misogynist language on Twitter (and other online social spaces)2016.
- 32. Anzovino M, Fersini E, Rosso P, editors. Automatic identification and classification of misogynistic language on twitter2018: Springer.
- 35. Becker M. Patriarchy and inequality: Towards a substantive feminism. U Chi Legal F. 1999:21.
- 36. Manne K. Down girl: The logic of misogyny: Oxford University Press; 2017.
- 37. Dehingia N, Lundgren R, Dey AK, Raj A. Trends in online misogyny before and during the COVID-19 pandemic: Analysis of Twitter data from five South-Asian countries. Center on Gender Equity and Health2021. p. 1–4.
- 38. Siegel A, Sterling J, Pullen B, Bonneau R, Nagler J, Tucker J. Trumping Hate on Twitter? Online Hate Speech and White Nationalist Rhetoric in the 2016 US Election Campaign and its Aftermath. 2017.
- 41. Dey L, Chakraborty S, Biswas A, Bose B, Tiwari S. Sentiment analysis of review datasets using naive bayes and k-nn classifier. arXiv preprint arXiv:161009982. 2016.
- 42. Joachims T, editor Text categorization with support vector machines: Learning with many relevant features. European conference on machine learning; 1998: Springer.
- 43. Devlin J, Chang M-W, Lee K, Toutanova K. Bert: Pre-training of deep bidirectional transformers for language understanding. arXiv preprint arXiv:181004805. 2018.
- 50. Anita Gurumurthy, Chami N. Digital India as if women matter: A policy discussion paper. India Office of the Heinrich Böll Foundation; 2018.
You are using an outdated browser. Upgrade your browser today or install Google Chrome Frame to better experience this site.

- IMF at a Glance
- Surveillance
- Capacity Development
- IMF Factsheets List
- IMF Members
- IMF Timeline
- Senior Officials
- Job Opportunities
- Archives of the IMF
- Climate Change
- Fiscal Policies
- Income Inequality
Flagship Publications
Other publications.
- World Economic Outlook
- Global Financial Stability Report
- Fiscal Monitor
- External Sector Report
- Staff Discussion Notes
- Working Papers
- IMF Research Perspectives
- Economic Review
- Global Housing Watch
- Commodity Prices
- Commodities Data Portal
- IMF Researchers
- Annual Research Conference
- Other IMF Events
IMF reports and publications by country
Regional offices.
- IMF Resident Representative Offices
- IMF Regional Reports
- IMF and Europe
- IMF Members' Quotas and Voting Power, and Board of Governors
- IMF Regional Office for Asia and the Pacific
- IMF Capacity Development Office in Thailand (CDOT)
- IMF Regional Office in Central America, Panama, and the Dominican Republic
- Eastern Caribbean Currency Union (ECCU)
- IMF Europe Office in Paris and Brussels
- IMF Office in the Pacific Islands
- How We Work
- IMF Training
- Digital Training Catalog
- Online Learning
- Our Partners
- Country Stories
- Technical Assistance Reports
- High-Level Summary Technical Assistance Reports
- Strategy and Policies
For Journalists
- Country Focus
- Chart of the Week
- Communiqués
- Mission Concluding Statements
- Press Releases
- Statements at Donor Meetings
- Transcripts
- Views & Commentaries
- Article IV Consultations
- Financial Sector Assessment Program (FSAP)
- Seminars, Conferences, & Other Events
- E-mail Notification
Press Center
The IMF Press Center is a password-protected site for working journalists.
- Login or Register
- Information of interest
- About the IMF
- Conferences
- Press briefings
- Special Features
- Middle East and Central Asia
- Economic Outlook
- Annual and spring meetings
- Most Recent
- Most Popular
- IMF Finances
- Additional Data Sources
- World Economic Outlook Databases
- Climate Change Indicators Dashboard
- IMF eLibrary-Data
- International Financial Statistics
- G20 Data Gaps Initiative
- Public Sector Debt Statistics Online Centralized Database
- Currency Composition of Official Foreign Exchange Reserves
- Financial Access Survey
- Government Finance Statistics
- Publications Advanced Search
- IMF eLibrary
- IMF Bookstore
- Publications Newsletter
- Essential Reading Guides
- Regional Economic Reports
- Country Reports
- Departmental Papers
- Policy Papers
- Selected Issues Papers
- All Staff Notes Series
- Analytical Notes
- Fintech Notes
- How-To Notes
- Staff Climate Notes
Geopolitics and its Impact on Global Trade and the Dollar
First Deputy Managing Director Gita Gopinath Series on the Future of the International Monetary System (IMS) Stanford Institute for Economic Policy Research
May 7, 2024
AS PREPARED FOR DELIVERY
Global economic ties are changing in ways we have not seen since the end of the Cold War.
After years of shocks—including the COVID-19 pandemic and Russia’s invasion of Ukraine—countries are reevaluating their trading partners based on economic and national security concerns. Foreign direct investment flows are also being re-directed along geopolitical lines. Some countries are reevaluating their heavy reliance on the dollar in their international transactions and reserve holdings.
All of this is not necessarily bad. Given the recent history of events, policymakers are increasingly—and justifiably—focused on building economic resilience. But if the trend continues, we could see a broad retreat from global rules of engagement and, with it, a significant reversal of the gains from economic integration.

Let’s take a closer look at how far we have gone down that route already. New trade restrictions have increased sharply—more than tripling since 2019—while financial sanctions have also expanded. The geopolitical risk index has spiked in 2022 following Russia’s invasion of Ukraine.
And private sector concerns about fragmentation—gauged by the number of mentions in corporate earnings calls—have surged.

Despite these trends, there are not yet clear signs of deglobalization at the aggregate level. Since around the time of the global financial crisis, when the 1990s-early 2000s hyper-globalization came to an end, the ratio of goods trade to GDP has been roughly stable—fluctuating between 41 and 48 percent.
But under the surface, there are increasing signs of fragmentation. Trade and investment flows are being redirected along geopolitical lines.
For example, China’s share in U.S. imports declined by 8 percentage points between 2017 and 2023 following a flare-up in trade tensions. During the same period, the U.S. share in China’s exports dropped by about 4 percentage points.
And direct trade between Russia and the West collapsed following the invasion of Ukraine and subsequent sanctions on Russia.

What about the implications of geopolitics for trade relations more broadly?
Consider a world divided into three blocs: a U.S. leaning bloc, a China leaning bloc, and a bloc of nonaligned countries.
The average weighted quarter-on-quarter [1] trade growth between U.S. leaning countries and China leaning countries during 2022Q2 – 2023Q3 was almost 5 percentage points lower than the average quarterly weighted trade growth during 2017Q1 – 2022Q1.
At the same time, quarterly growth in trade within blocs only saw a 2-percentage point drop.
On average in the period after Russia’s invasion of Ukraine, we see that trade and FDI between blocs declined by roughly 12 and 20 percent more than flows within blocs, respectively.
It is notable that these patterns are not driven uniquely by the U.S. or China and hold up even when you take these two countries out of the picture.
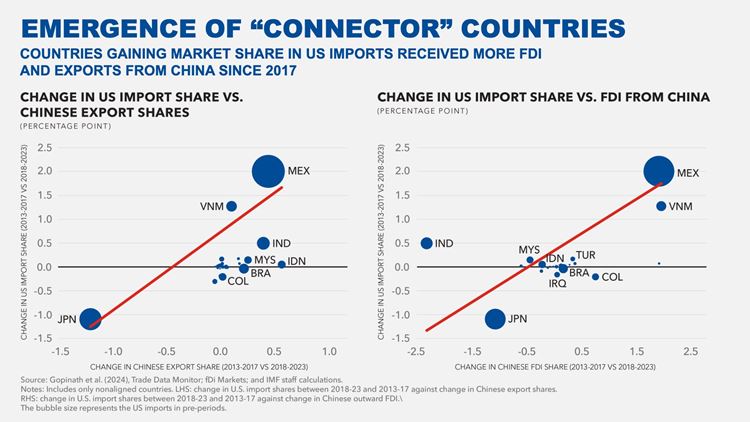
This begs a question: Why have we not seen an even bigger impact of de-coupling between geopolitical rivals on global trade?
This is because some trade and investment are being re-routed through third-party countries, partially offsetting the erosion of direct links between the U.S. and China. Since 2017, greater Chinese presence in a country—measured either through exports or announced greenfield investment—has been associated with increased exports of that country to the U.S.
The emergence of these “connector” countries—perhaps most notably Mexico and Vietnam—may have helped cushion the global economic impact of direct trade decoupling between the U.S. and China. But whether it has helped to diversify exposures and increase supply chain resilience remains an open question.
The path forward will depend on policymakers. They may accept such rerouting of trade and FDI in order to preserve some of the gains of economic integration. Or they may continue to raise barriers for cross-border trade and investment, further breaking both direct and indirect links between politically distant countries.
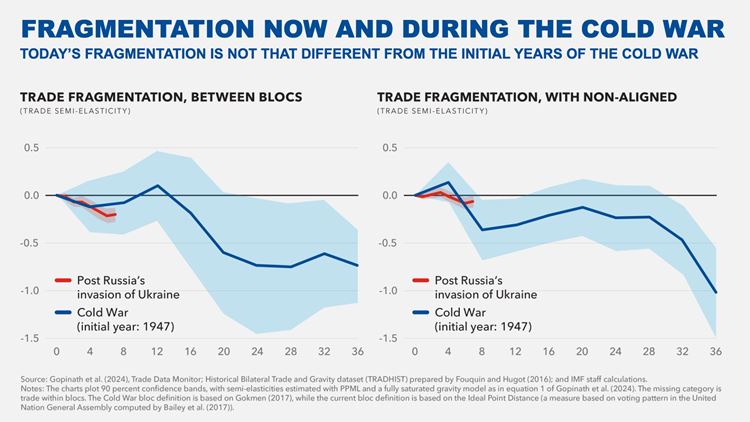
How bad could it get?
To gauge the potential magnitude of fragmentation along geopolitical lines, let’s compare the current trade fragmentation with that of the Cold War period.
Trade between the rival Western and Eastern blocs was significantly depressed during the Cold War, relative to trade within these blocs.
Thus far, today’s fragmentation is not significantly different from the initial years of the Cold War. However, compared to the average “between-bloc trade shortfall” during the entire Cold War period, fragmentation so far is an order of magnitude smaller.
But there is still cause for concern. Trade fragmentation is much more costly this time around because unlike the start of the Cold War when goods trade to GDP was 16 percent, now that ratio is 45 percent. Moreover, while back then countries within a bloc were taking off trade restrictions, now we are in an environment of growing protectionism with several countries turning inward.
The potential role of non-aligned countries in the current trade frictions also makes the situation today different from the Cold War experience. The evidence suggests such countries did not play an important role serving as connectors between rival blocs during the Cold War—likely because they had a much smaller economic footprint and global supply chains were not yet developed. Today, they have greater economic and diplomatic heft and are much more integrated into the global economy. Their role as connectors this time round can help attenuate some of the costs of fragmentation.

Have geopolitical tensions and the shifting patterns of trade and FDI affected the currency composition of cross-border payments and FX reserves?
Data on currency use in international trade and finance is sparser and comes with longer lags than trade figures. Even so, we are so far not seeing a significant impact. Despite increased geopolitical risks, the latest data show that the U.S. dollar remains dominant. According to SWIFT, it accounts for over 80 percent of trade finance, likely because much of commodity trade continues to be invoiced and settled in dollars.
It also accounts for nearly 60 percent of FX reserves despite the gradual diversification of FX reserves away from the dollar and partly into non-traditional reserve currencies such as the Australian dollar, and the Canadian dollar. [2]

Given the reshaping of trade relations, has the currency composition of trade finance changed during 2022-23?
The answer is not much for U.S.-leaning countries, but there have been more visible changes for China-leaning countries.
For the China bloc, the USD share of trade finance payments has declined since early 2022. At the same time, the RMB share has more than doubled, from around 4 percent to 8 percent.
This is not a Russia only story. In fact, the share of RMB in trade finance for the China bloc would be only slightly lower if Russia were excluded from it. Most RMB denominated trade finance captured in the SWIFT data reflects transactions between China and China leaning countries.
For China, the share of RMB in all cross-border transactions of Chinese non-bank entities with foreign counterparts was close to zero 15 years ago but has risen to reach around 50 percent in late 2023. In contrast, the USD share has been on a declining trend, falling from around 80 percent in 2010 to 50 percent in 2023.
The increasing use of the RMB may have been supported by the Cross-Border Interbank Payments System (CIPS)—a system launched by the People’s Bank of China which offers clearing and settlement services for cross-border transactions in RMB.

Looking at global FX reserves, the most notable development during 2022-23 has been an increase of gold purchases by central banks.
Gold is generally viewed as politically neutral safe asset, which can be stored at home and be insulated from sanctions or seizure. It can also be an inflation hedge but cannot be easily used in transactions.
The share of gold in the FX reserves of the China bloc has been rising since 2015—a trend not exclusively driven by China and Russia. Importantly, during the same period, the share of gold in FX reserves of countries in the U.S. bloc has been broadly stable.
This suggests that gold purchases by some central banks may have been driven by concerns about sanctions risk. This is consistent with a recent IMF study [3] confirming that FX reserve managers tend to increase gold holdings to hedge against economic uncertainty and geopolitical including sanctions risk.
Looking at China, the share of gold in total FX reserves has increased from less than 2 percent in 2015 to 4.3 percent in 2023. During the same period, the value of China’s holdings of U.S. Treasury and Agency bonds relative to FX reserves has declined from 44 percent to about 30 percent. This reflects both net purchases and valuation effects.
The downward trend holds even if we account for the fact that some of China’s holdings of U.S. bonds may be held in Belgium (Euroclear), as some analysts suggest. [4]
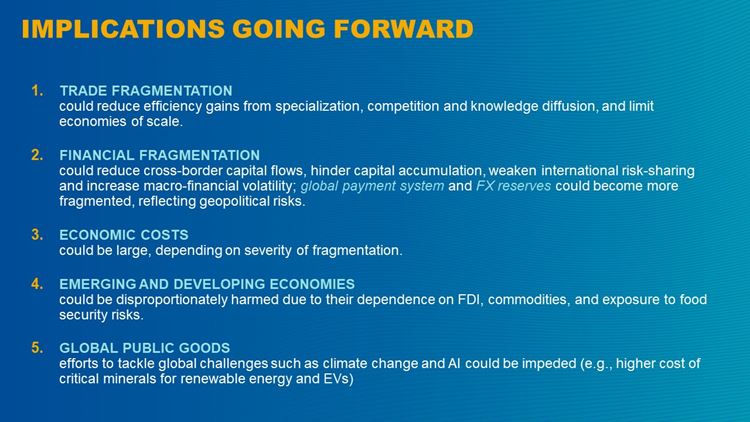
If fragmentation deepens, what would be the economic cost? And how will those costs be transmitted?
Trade is the main channel through which fragmentation could reshape the global economy. Imposing restrictions on trade would diminish the efficiency gains from specialization, limit economies of scale, and reduce competition. The capacity of trade to incentivize within-industry reallocation and generate productivity gains would be stifled. Less trade would also imply less knowledge diffusion, a key benefit of integration, which could also be reduced by fragmentation of cross-border direct investment. A useful example is Brexit. Because of the extensive interlinkages between Europe and the UK, Brexit is thought to have had a sizable negative effect on the UK economy.
There would also be costs from financial fragmentation. It would limit capital accumulation—because FDI would be reduced—and affect the allocation of capital, asset prices, and the international payment system. Financial fragmentation could also lead to weaker international risk sharing, resulting in higher macro-financial volatility for individual countries, and higher crisis risks due to idiosyncratic shocks [5] . The global payment system could become fragmented along geopolitical lines with the emergence of new payment platforms with limited or no interoperability. This could lower efficiency, and lead to fragmented standards and regulation.
In addition, FX reserves could be re-aligned to reflect new economic links and geopolitical risks. A global system with multiple reserve currencies could have several benefits, including a larger pool of safe assets and more opportunities for FX reserve diversification. But the stability of such a system would be at risk without strong policy coordination among all reserve currency issuing countries—including through a network of swap lines. This would not be possible if the world is divided along geopolitical lines.
The estimates of the economic costs of fragmentation vary widely and are highly uncertain. In a mild scenario with low adjustment costs, losses could be as low as 0.2% of world GDP, while in an extreme trade fragmentation scenario with limited ability of economies to adjust, losses could be as high as 7 percent of global GDP [6] . As for foreign direct investment, fragmentation in a world divided into two blocs centered around the U.S. and China with some countries remaining non-aligned could result in long term losses of around 2 percent of global GDP [7] .
Some countries could benefit from fragmentation in its mild forms. But if fragmentation worsens, they could be left with a larger slice of a much smaller pie. In short, everyone could lose.
Some emerging and developing economies could benefit from fragmentation in its mild forms as trade and FDI gets redirected towards them. However, as a group they would be disproportionately negatively impacted by more severe forms of fragmentation. These economies rely more on imports and exports of key products, including commodities, for which it is harder and more costly to find new markets and suppliers.
Our research suggests that low-income countries, on average, could experience 4 times the simulated global economic output loss of other countries in the event of fragmentation of commodity markets into two blocs [8] . Most of the losses would be due to trade restrictions of agricultural commodities, as low-income countries are heavily dependent on agricultural imports to feed their populations, raising concerns about food security in poorer countries.
Furthermore, emerging markets and developing economies are heavily dependent on FDI from advanced economies, the main source of global investment. They would also be left without positive spillovers from FDI to local firms in the case of friend-shoring or reshoring, when FDI is relocated to “friendly” countries in the other bloc or home.
Fragmentation would also inhibit our efforts to address other global challenges that demand international cooperation. The breadth of these challenges—from climate change to AI—is immense.
Recent IMF analysis shows that fragmentation of trade in minerals critical for the green transition—such as copper, nickel, cobalt, and lithium—would make the energy transition more costly. Because these minerals are geographically concentrated and not easily substituted, disrupting their trade could lead to sharp swings in their prices, suppressing investment in renewables and EV production.

So, what can we do to prevent this? The ideal solution would be to preserve and strengthen the multilateral rules-based global trading system and the international monetary system.
Strengthening the trading system would require restoring a fully functioning WTO dispute settlement mechanism. It will also require making more progress on dealing with subsidies and national security trade restrictions and developing international rules and norms on the appropriate use and design of industrial polices.
To strengthen the international monetary system, concerted efforts are needed to prevent fragmentation of the global payment system and related standards and regulations. We also need to ensure a well-resourced and efficient global financial safety net, improve measurement and monitoring of cross-border crypto flows, and maintain global dialogue on debt restructuring.
But given where we are today, the ideal may be difficult to achieve. Therefore, we need pragmatic steps to rebuild trust.
The first step is to keep open the lines of communication and stay engaged. Dialogue between the U.S. and China—which we are now seeing—can help prevent the worst outcomes from occurring.
Non-aligned countries can also play a bigger role—using their economic and diplomatic heft to keep the world integrated.
The second pragmatic step is to work together on areas of common interest. Take climate, for example. Over 70 countries have come together through the WTO’s Trade and Environmental Stability Structured Discussions to identify opportunities to promote the trade of renewable energy goods and services.
We also see progress in services and digital trade. Policy restrictions are high in these fast-growing areas of the global economy. But recognizing this, 90 countries representing more than 90 percent of global trade are working together toward common digital trade rules.
And 71 members came together around a WTO plurilateral agreement on Services Domestic Regulation that aims to promote more transparent, predictable, and efficient regulatory frameworks and is expected to reduce services trade costs by USD 127 billion.
In addition, the G20 is working on interlinking cross-border payment systems, aiming to improve efficiency and reduce transaction costs.
The third step is to limit harmful unilateral policy actions—including industrial policies. While it is appropriate to try to correct market failures through policy interventions, it must be carefully handled. Politically, industrial policies may be hard to limit or roll back given their concentrated benefits and diffused costs. History is replete with cautionary tales of policy mistakes, high fiscal costs & negative spillovers to other countries. Internationally, such policies have led to retaliation, which would deepen fragmentation.
Adhering to existing legal frameworks is also critical for maintaining trust between countries and in the international monetary system.
For example, many countries are following closely the ongoing discussion about potential use of Russian state assets, including reserves of the Bank of Russia, to support Ukraine. While this is for relevant courts and jurisdictions to determine, for the IMF, it is important that any action has sufficient legal underpinnings and does not undermine the functioning of the international monetary system.
While rebuilding trust is difficult and may take time, it is critical to avoid the worst outcomes in a rapidly fragmenting world. It is well worth it to preserve some of the enormous gains from economic integration that have made the world more prosperous and more secure.
[1] See Gopinath at al “Changing Global Linkages: A New Cold War?”, IMF Working Paper No. 2024/076 ( link )
[2] See Arslanalp et al. “The Stealth Erosion of Dollar Dominance: Active Diversifiers and the Rise of Nontraditional Reserve Currencies” IMF Working Paper, No. 2022/058 ( link )
[3] Arslanalp et al “Gold as International Reserves: A Barbarous Relic No More?”, IMF Working Paper No. 2023/014 ( link ) analyze a panel of 144 economies over the period 1980-2021.
[4] Analysts believe that part of the US securities holdings attributed to Belgium may belong to other countries, such as China or Saudi Arabia (see Bertaut and Judson (2014), Sester (2016)).
[5] See GFSR April 2023 “Safeguarding Financial Stability Amid High Inflation and Geopolitical Risks” ( link )
[6] See IMF Staff Discussion Note, “Geoeconomic Fragmentation and the Future of Multilateralism”, January 2023 ( link )
[7] See WEO April 2023, Chapter 4 “Geoeconomic Fragmentation and Foreign Direct Investment” ( link )
[8] See WEO October 2023, Chapter 3 “Fragmentation and Commodity Markets: Vulnerabilities and Risks” ( link )
IMF Communications Department
Media relations.
PRESS OFFICER:
Phone: +1 202 623-7100 Email: [email protected]
@IMFSpokesperson
IMAGES
VIDEO
COMMENTS
The World Health Organization had classified COVID 19 as a public health emergency of global significance due to its widespread presence throughout the world. On March 11, 2020, the World Health Organization (WHO) proclaimed COVID 19 to be a pandemic after cases were confirmed in several nations. A virus from the family of coronaviruses is what ...
The CDC reports that the percentage of adults who reported symptoms of anxiety of depression in the past 7 days increased from 36.4 to 41.5 % from August 2020 to February 2021. Other reports show that having COVID-19 may contribute, too, with its lingering or long COVID symptoms, which can include "foggy mind," anxiety, depression, and post ...
The COVID-19 pandemic is far from over and could yet evolve in unanticipated ways, but one of its most important lessons is already clear: preparation and early execution are essential in ...
Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus. Most people infected with the virus will experience mild to moderate respiratory illness and recover without requiring special treatment. However, some will become seriously ill and require medical attention. Older people and those with underlying medical ...
The World Health Organization is the global coordinating agency for the response to the COVID-19 pandemic. The Organization works with Member States and partners on all aspects of the pandemic response, including facilitating research, developing guidance, coordinating vaccine development and distribution, and monitoring daily case numbers and ...
About this speech. Joe Biden. September 09, 2021. Source The White House. As the Delta variant of the Covid-19 virus spreads and cases and deaths increase in the United States, President Joe Biden announces new efforts to fight the pandemic. He outlines six broad areas of action--implementing new vaccination requirements, protecting the ...
Speeches and Remarks. South Court Auditorium. Eisenhower Executive Office Building. 12:54 P.M. EDT. THE PRESIDENT: Good afternoon. I've just been briefed by my COVID-19 team on the progress we ...
Biden on the Anniversary of the COVID-. 19. Shutdown. Briefing Room. Speeches and Remarks. East Room. 8:01 P.M. EST. THE PRESIDENT: Good evening, my fellow Americans. Tonight, I'd like to talk ...
It connected us in a way, it showed us that we should all stick together. During this chaos, while many of us in a panic, it showed us the weight of humanity. It reminded us who we are. Maybe the world will finally change. We humans are fragile by ourselves. Our strength lies in being part of a community.
The coronavirus pandemic presents a challenge the world has not faced-on this scale-for generations. It's often said that extraordinary times call for extraordinary measures, and we are witnessing every day the heroic efforts of physicians, nurses, medical workers, public health professionals, and the public to manage the enormity of ...
The COVID-19 pandemic has presented an unprecedented global challenge, and in the face of this crisis, many countries have debated the implementation of vaccination mandates. ... Check out some examples of persuasive speeches on Covid-19: Persuasive Speech About Covid-19 Example. Persuasive Speech About Vaccine For Covid-19. Expert Tip.
WHO Director-General's opening remarks at the media briefing on COVID-19 - 20 March 2020. Good morning, good afternoon and good evening, wherever you are. Every day, COVID-19 seems to reach a new and tragic milestone. More than 210,000 cases have now been reported to WHO, and more than 9,000 people have lost their lives.
The COVID-19 Pandemic — Finding Solutions, Applying Lessons Learned (Remarks as prepared for delivery. The text and video of this speech are slightly, though not substantively different from the ...
The Covid-19 pandemic is one of the most dangerous challenges this world has faced in our lifetime. It is above all a human crisis with severe health and socio-economic consequences. The World ...
ridahussain86. report flag outlined. The 2019-20 coronavirus pandemic is an ongoing pandemic of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).Coronavirus disease (COVID-19) is an infectious disease caused by a newly discovered coronavirus. • Avoid visitors while you have symptoms.
The COVID-19 global health emergency and its economic and social impacts have disrupted nearly all aspects of life for all groups in society. People of different ages, however, are experiencing its effects in different ways. Based on survey findings from 90 youth organisations from 48 countries, this policy brief outlines practical measures governments can take to design inclusive and fair ...
The days dragged on in my apartment, in black and white, like my photos. Sometimes we tried to smile, imagining that I was asymptomatic, because I was the virus. Our smiles seemed to bring good ...
People have long turned to creative expression in times of crisis. During the coronavirus pandemic, artists are continuing to illustrate, play music, dance, perform — and write poetry.
Background. The coronavirus (COVID-19) pandemic has had diverse negative psychological effects globally. Individuals have experienced a wide range of adversities due to the virus, including those relating to the virus itself (such as experiencing illness oneself, concerns for friends and family, and bereavement), financial adversities (including loss of work or income, and inability to pay ...
COVID-19: Emergence, Spread, Possible Treatments, and Global Burden. The Coronavirus (CoV) is a large family of viruses known to cause illnesses ranging from the common cold to acute respiratory tract infection. The severity of the infection may be visible as pneumonia, acute respiratory syndrome, and even death.
1. Introduction. The outbreak of the coronavirus disease 2019 (COVID-19) has emerged as the largest global pandemic ever experienced [].Experts have proposed that social lockdown will lead to improvements such as controlling the increase in the number of infected individuals and preventing a huge burden on the healthcare system [, , ].Governments of many countries across the world have ...
But that picture was dramatically altered with the onset of the COVID-19 pandemic. Efforts to contain the spread of the virus caused a sudden stop in economic activity during March and April. While the extent of the closures and shutdowns varied widely throughout the country, the sudden loss of employment and the contraction in output were like ...
A new study by Concordia University in Canada found that consumers largely panic-bought during the COVID-19 pandemic, and lessons that could be learned for future events.
To the Case Western Reserve University community, Commencement marks the culmination of years of hard work and dedication in classrooms, labs, clinicals, internships, extracurriculars and so much more. Though this always is one of our favorite events of any year, we are especially looking forward to this year's festivities, as many members of the undergraduate Class of 2024 had their high ...
19. Pandemic. Briefing Room. Speeches and Remarks. 5:02 P.M. EDT. THE PRESIDENT: Good evening, my fellow Americans. I want to talk to you about where we are in the battle against COVID-19, the ...
From the COVID-19 pandemic to LGBTW Pride Month to President Joe Biden, Butker had plenty to say about all of the above. And his traditional Catholic values certainly shined through throughout the ...
As early as May 2020, the United Nations Secretary General made a global appeal to tackle COVID-19 influenced hate speech on digital platforms, ... Raj A. Trends in online misogyny before and during the COVID-19 pandemic: Analysis of Twitter data from five South-Asian countries. Center on Gender Equity and Health2021. p. 1-4. 38.
Nigel Farage: We must be prepared to leave WHO over pandemic treaty 'Expensive, unelected, unaccountable' World Health Organisation has gone past its remit if it forces lockdowns on nations ...
After years of shocks—including the COVID-19 pandemic and Russia's invasion of Ukraine—countries are reevaluating their trading partners based on economic and national security concerns. Foreign direct investment flows are also being re-directed along geopolitical lines. Some countries are reevaluating their heavy reliance on the dollar in their international transactions and reserve ...
We must stop the pandemic treaty and take back control from the WHO A health Warning" to the bureaucrats in Geneva: ignore us and a second Brexit will be on the cards